Download
1 / 41
440 likes | 512 Views
Learn about Acute Rheumatic Fever (ARF), an immuno-inflammatory condition that affects the heart and joints, often triggered by streptococcal infection. Explore its epidemiology, pathology, clinical features, diagnosis, sequelae, and treatment options.

E N D
ACUTE RHEUMATIC FEVER DR SHYAM SUDHIR PROFESSOR YMC
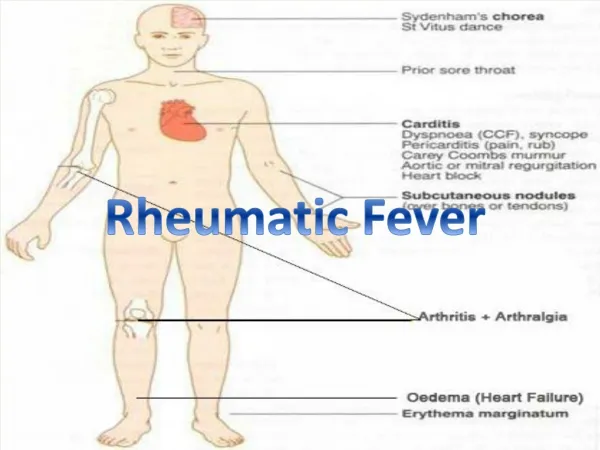
“Licks the joint, bites the heart” • Acute ARF is an immuno-inflammatory condition that presents as a connective tissue disease, clinically manifesting as carditis & arthritis, sometimes with chorea, subcutaneous nodules & erythema marginatum. • An untreated Group- A beta hemolytic streptococcal infection is the commonest antecedent event that precipitates an attack of ARF.
Introduction • A multisystem, immunologically mediated inflammatory disease • As a delayed sequel to group A Beta hemolytic streptococcal (GAS) infection. • Leading cause of Cardiovascular disease • Incidence : Peak 5 – 15 yrs
Epidemiology • Prevalence of RHD in India in the vulnerable age group 5-15 years is not less than 0.5 %. • About 50% of children with ARF will suffer from RHD
Studies show a dramatic decline in developed countries A- antibiotic coverage has increased B- Better housing C- Conditions ( economic & health) have improved D- Decreased bacterial virulence E- Easy access to medical care
Pathology & Pathogenesis ARF is preceded by - Pharyngitis due to Group A streptococcus rheumatogenic stains Pathogenesis- two important theories Cytotoxicity theory Immunologic theory
Pathology It is an acute non suppurative, involving the connective or collagen tissue. Disease process is diffuse, but it primarily involves the heart,joints, skin & brain. Typical histological lesion- ‘Ashoff’ bodies ARF - First attack - Recurrence Valvular lesions- small verrucae- borders of valves- scar tissue
Myocardial Aschoff body – the cells are large, elongated, with large nuclei; some are multinucleate
Clinical features & diagnosis Jones criteria (updated in 1992) 5- Major 4- Minor 2 majors or 1major & 2 minors with Evidence of (microbiologic or serologic) of recent Group A beta hemolytic streptococcal infection
Carditis Polyarthritis Erythema marginatum Subcutaneous nodules Chorea Pnemonic C2ASE C – Carditis C – Chorea A – Arthritis S – Subcutaneous nodules E – Erythema marginatum Majors
Minors Clinical features • Fever • Arthralgia (in the absence of polyarthritis) Laboratory features • Elevated acute phase reactants • Raised ESR • Raised CRP • Prolonged PR interval
3 Circumstances – Where ARF diagnosed without strict adherence to Jones criteria • Indolent carditis may be sole manifestation • Chorea may be the sole manifestation • ARF recurrence may not fulfill the Jones criteria
Arthritis • Migratory polyarthritis • No sequelae • Tender • Dramatic response to small dose of salicylate
Carditis • Pancarditis- exudative Pericarditis variable myocarditis variable Endocarditis (valvulitis) Murmur (valvular insufficiency) Sequale may be present in 50% of children Outcome - Complete recovery - Morbidity - Mortality
Carditis Schematic representation of the aetiopathogenic events occurring during the development of carditis
Chest radiograph of an 8 year old patient with acute carditis before treatment
Chest radiograph of an 8 year old patient with acute carditis after treatment
Carditis presentation • Tachycardia out of proportion to fever sleeping pulse rate raised • Pericardial rub • CCF, gallop rhythm and so on • Cardiac enlargement Reversible • Pulmonary hypertension • Cardiac murmur Irreversible }
Murmur • High pitched apical holosystolic murmur radiating to axilla – Mitral regurgitation • An apical mid diastolic murmur • A high pitched decrescendo diastolic murmur- upper sternal border- Aortic regurgitation
Carditis sequelae ( chronic) Mitral insufficiency • Some loss of valvular substance • Shortening & thickening of Chordae tendinae Mitral stenosis • Takes longer duration to develop after an attack of ARF • Fibrosis of mitral ring, commissural adhesions • Contracture of the valve leaflets, chordae & papillary muscles • Opening snap, low pitched, rumbling mitral diastolic murmur with pre systolic accentuation ending in loud first sound
Carditis sequelae (chronic) – Contd.. Aortic insufficiency • Sclerosis of aortic valve- distortion & retraction of the cup • Characteristic cardiac murmur, early diastolic • An apical pre systolic murmur ( Austin flint)
Investigation • X ray chest • ECG • ECHO • Doppler • Catheterization studies
Differential diagnosis • Arthritis- Rheumatic arthritis (JRA) - SLE - Reactive arthritis – shigella, Salmenolosis, Yersenia - Lyme’s disease • Carditis- viral myocarditis,& Pericarditis Infective endocarditis Congenital heart lesions • Chorea - Huntington chorea Wilson disease Tics
Treatment • Rest- Absolute bed rest if carditis present • Antibiotics- regardless of throat culture 10 days of oral penicillin or erythromycin or Single Benzathine penicillin IM • Anti inflammatory therapy- Carditiswithout Cardiomegaly & or CCF Aspirin:100mg/Kg/24hr qid 4 days 75 mg/24hrs/ qid 4 week
Treatment – Contd.. • Carditis with cardiomegaly & or CCF Prednisolone 2mg/Kg/24hrs qid 2-3 Wk followed by tapering by 5mg every 2-3days At the beginning of tapering Prednisolone, start Aspirin 75mg/Kg/day/qid for 6 Wk
Treatment – Contd.. • Supportive therapy- when required Digoxin, Diuretics, Oxygen, Fluid & salt restriction • Chronic heart lesions Prophylaxis against bacterial endocarditis during surgical procedures
Sydenham’s chorea • 10 – 15 % of patients • Usually a delayed and often the sole manifestation of acute rheumatic fever • Characterized by involuntary movements, specially of the face and limbs, muscle weakness, disturbances of speech and gait, poor scholastic performance • Milk maid grip, spooning and pronation of extended hands, wormian movements of tongue
Sydenham’s chorea - Treatment • Anti inflammatory agents usually not required • Phenobarbitol 15-30 mg tds or qid oral is the drug of choice • Haloperidol 0.01- 0.03mg/kg/24hrs bd oral • Chlorpromazine 0.5mg/kg every 4-6 hrs oral
Erythema marginatum • Rare • Erythematous, serpiginous, macular rash with pale centres • NON PRURITIC, NO INDURATION • Seen over trunks and extremities
Erythema marginatumon the trunk, showing erythematous lesions with pale centers and rounded or serpiginous margins
Subcutaneous nodules • Small, pea sized, 0.5 to 2 cms in diameter • Firm, mobile, PAINLESS • Seen over the extensor surface of WRIST, ELBOW, SPINE • Usually seen in individuals with long standing carditis
Subcutaneous nodule on the extensor surface of elbow of a patient with acute rheumatic fever
Sydenham’s chorea • Long latent period • Uncontrollable movements • Facial grimacing • In coordination • Poor school performance • Emotional liability • Exacerbated by stress • Disappearing sleep • Rarely leads to permanent neurological sequeale
Primary Prophylaxis Vulnerable children from 5 to 15 yrs with pharyngitis Oral • Penicillin 250 -500mg bd/tds 10 days • Erythromycin 20- 40 mg/kg/day tds/qid- 10 days • First generation Cephalosporin- 10 days • Azithromycin 12mg/kg/day single dose – 5days maximum 500mg/day Parentral • < than 27kg single dose IM Benzathine penicillin 6,00,000 U • > than 27kg single dose IM Benzathine penicillin 1,20,0000 U Therapy instituted before 9th day of symptoms of acute Pharyngitis
Secondary prophylaxis Duration from 5 yrs to life long depending upon severity
Fill in the blanks • RF caused by________ organism,and name the common strains responsible for it__________ • Prevalence of RF is most vulnerable between _______ age group • Name the criteria used for diagnosis of initial attack of RF ________ • Primary prophylaxis with pencillin is given for ____ days
Carditis is treated with _____? • Carditis with CCF treated with ____and followed by ____ ? • _____valve is commonly affected in RHD? • Dose of Benzathinepencilline below 27kg is ____? • Dose of benzathinepencilline above 27 kg is ____? • Benzathinepencilline is given in _____prophylaxis? • Benzathinepencilline is given once in how many days or weeks?_____
QUESTION • What is the diagnostic criteria for rheumatic fever? • How do you treat reumaticcarditis with CCF? • Tertiary prophylaxis in RF? • Prophylaxis of infective endocarditis in RHD? • Management of acute RF • Digoxin in cardiac failure • What is the mechanism of action and side effects of pencillin?
Primary prevention of rheumatic fever? • Treatment of CCF? • Discuss management of child with rheumatic carditis ? • Rheumatic carditis? • Subcutaneous nodule? • Sydenham’s chorea? • Modified jone’s criteria?