Download

1 / 200
2.03k likes | 2.54k Views
RHEUMATIC FEVER. Acute rheumatic fever is a non-infectious delayed complication of streptococcal sore throat due to Group A Beta hemolytic streptococcus (GABHS). HISTORY. Historical evidence is clouded probably because of multisystemic disease RF is relatively recent

E N D
Acute rheumatic fever is a non-infectious delayed complication of streptococcal sore throat due to Group A Beta hemolytic streptococcus (GABHS)
HISTORY • Historical evidence is clouded probably because of multisystemic disease • RF is relatively recent • Crowded and poor working conditions fostered by Industrial revolution contributed to spread of RF • World War II was associated with ravaging epidemics
EPIDEMIOLOGY • Incidence of rheumatic fever and RHD ( rheumaticheartdisease) has decreased in the United States and other industrialized countries during the past 80 years. Prevalence of RHD in the United States is now less than 0.05 per 1000 population • Worldwide, an estimated 5-30 million children and young adults have chronic RHD, and 90,000 patients die from this disease each year.
Incidence • The incidence of RF in Developing countries is 27-100/1 mil /yr • In developed countries is <5/ 1mil/yr (G.S.Sainani Japi 2006)
Area Prevalence/1000 • US 0.3 • Japan 0.3 • India 2.2 • Africa 5.7 • South America 1.3
Pathogenesis RF occurs 1-5wks after streptococcal throat infection avg is 3 wks • Streptococci-GABHS ( group A beta haemolitic streptococcus) • Gram positive cocci occuring in chains • Capsulated with fimbria
STREPTOCOCCI • Streptococci pyogenes • Beta Haemolytic-Complete haemolysis on blood agar • Lancefield groups 19 –according to carbohydrate antigen ( A to U except I,J) • Surface M protein -80 serotypes • T,R proteins.
GABHS Rheumatogenic serotypes 1,3,5,6,14,12,18,19,24,27,29 Nephritogenic serotypes 12 , 49
structure • Capsule hyaluronic acid • Cellwall • Outer –fimbria+lipoteichoic acid+M protein • Middle-carbohydrate • Inner-peptidoglycan layer • Cytoplasmic membrane
Autoimmune disease; Antigenic mimicry Antibodies against these antigens result in a hyperactive immune response M protein helical protein-constant ,variable and highly variable region; M protein of GABHS virulence factor -> ability to resist phagocytosis Crossreactivity- cytoskeleton, tropomyosin and myosin. Group specific polysaccharide wall -> glycoprotein of cardiac valves Antibodies to the streptococcal peptidoglycan complexes have been implicated in rheumatic arthritis Somatic antigens of the cell wall & cell membrane -> myocardial sarcolemma ,vascular initima and skin In Sydenham chorea, antibodies directed against the cell membrane cross react with tissues in the caudate nucleus of the brain
TOXINS • Streptolysin(Hemolysin) O and S • Erythrogenic toxin • Streptokinase • DNAase • NADase • Hyaluronidase • Proteinase
STREPTOCOCCI • Throat,skin,URTI ( upper respiratory tract infections) • Isolated from 10-50% throat culture of healthy school children
PATHOLOGY • RF is a multisystem connective tissue disease • Inflammatory lesions in the heart, joints & subcutaneous tissue Microscopy • Aschoff granulomais the pathological hallmark of RF. It consists of central fibrinoid necrosis surrounded by histiocytes (Anitschkow cells) with a typical “owl-eye” nucleus.
Gross appearance Valves appear dull & thickened Verucous vegetations on the atrial surface of the mitral valve, chords, ventricular surface of aortic valve with edema or hemorrhage in the leaflet tissue Vegetations are composed of fibrin
Characteristics of Juvenile Rheumatic Mitral Stenosis • Fusion of cusps • severe Subvalvular fusion • Fixed fibrotic valve, no calcification • Mobile cusps with commissural fusion • Associated mild Mitral Regurgitation • Early & Severe pulmonary hypertension
Positive diagnosis of rheumatic fever • Sir T .Duckett Jones 1944 • Modified in 1956,1965,1984 and 1992
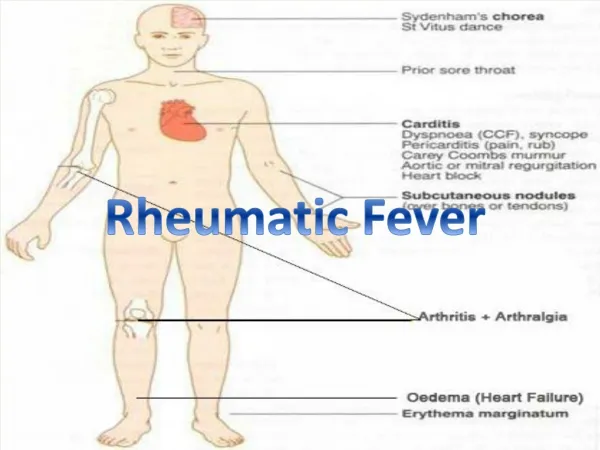
JONES CRITERIA 1992 MAJOR MANIFESTATIONS • Carditis • Polyarthritis • Chorea • Erythema marginatum • Subcutaneous nodules
MINOR MANIFESTATIONS Previous RF or RHD ( rheumatoidheartdisease) Clinical findings Athralgia Fever Lab findings Raised ESR Elevated C-reactive protein Prolonged PR interval
Supporting evidence of antecedent GABHS infection Positive throat culture or Rapid streptococcal antigen test Elevated or rising streptococcal antibody titer
Diagnosis of Rheumatic Fever • Two major manifestations OR One major & Two minor manifestations if supported by evidence of preceding GABHS infection indicate a high probability of Acute RF • Sensitivity 77%, Specificity 97%
Carditis • Seen in 42% of patients with acute RF • 80% of patients who develop carditis within the first 2 wks of onset of RF • Rheumatic carditis is a pancarditis affecting the endocardium, myocardium & pericardium to various degrees • Predominant effect is scarring of the heart valves
Endocarditis • Most commonly effects mitral & aortic valves • Mitral valve disease 70-75% pts of RHD • Mitral + Aortic valve disease 20-25% • Isolated Aortic valve disease 5-8% • Isolated Aortic stenosis is rare 3-4% (Kinare S G AIAMS 1972)
Isolated tricuspid & Pulmonary valve is never involved Tricuspid valve along with Mitral & Aortic valve is involved in 11.8% of RHD patients Rheumatic Pulmonary valve is very rare , if present it is quadrivalve
POLYARTHRITIS • Incidence > 2/3 rd of patients • Asymmetric, migratory involving large joints- knees, ankles, elbows & wrists • Axial joints are rarely involved • Swelling, redness ,hot, severe pain, limitation of joint movements are the main symptoms
Physical findings disproptionate to symptoms Joints are involved at various intervals lasts for 4-5 days Arthritis resolves by 3 to 4 wks without any permanent damage Joint aspirate >10000 WBCs/cu.mm Dramatic response to aspirin –improves within 48hrs
Differential diagnosis • Post streptococcal reactive arthritis • Septic arthritis • Gonococcal arthritis • Juvenile rheumatoid arthritis • Tuberculosis arthritis • Hepatitis B • Henoch-Scholein purpura • Serum sickness
CHOREA (St.Vitus dance) • It is a series of jerky, nonrepeatative, involuntary movements involving the face & extremities with emotional lability. • Movements disappear during sleep • Due rheumatic inflammation of basal ganglia & caudate nucleus • Late manifestation after several weeks (3mths or longer) after RF
SKIN MANIFESTATIONS • Subcutaneous nodules(1 to 21%) • Late manifestation of RF • Indicate presence of underlying carditis • Firm, painless, moveable 0.5 to 3cm in size • On bony prominence, extensor tendons (elbows,knees ,wrists,ankles), vertebral spinous process,suboccipital region,medial border of scapulae • Appear in crops, disappear in 8 to 12wks
Erythema Marginatum • Early or late manifestation • Incidence 10-15 % • Indicate presence of underlying carditis • On trunk & proximal extremities • Serpigenious erythrematous macular/papular nonpuritic rash • Rash extends outwards with central clearing • No residual scarring • May appear or disappear in mins-hrs
Laboratory Diagnosis Throat Culture • Positive in only 11% cases of ARF Streptococcal Antibody Tests ASLO Titer • Slide agglutination test • Elevated in 80% patients with ARF • Reach a maximum level 2-3wks after infection, plateau for 3-6mths & disappear in the next 6-12mths
Adults /preschool children < 85 todd units • School age = 170 todd units • Titers alter with age, geographical area • ASO titer >250 Todd units in adults >333 Todd units in children is used for diagnosis,
AntiDNAse B/Antihyaluronidase test • Done when ASO is nondiagnostic • Levels remain elevated for several mths • Less affected by antibiotics and steriods. • DNA ase 6-12 mths • Titre > 300 IU/dl
normal values Anti DNase B titer 1:60 unit in preschool, • 1:480 units in – school children & 1:340 in adults) • Antihyaluronidase > 200 IU/dl • Streptozyme test – 5 antigens • Rapid slide agglutination test
Acute phase reactants • Raised ESR • Elevated CRP ECG • Prolonged PR interval • Tachycardia • AV block • QRS-T changes s/o Myocarditis
Echocardiography • Helpful to diagnose silent carditis • More sensitive than clinical examination • 30% cardiac involvement in patients without clinical carditis
TREATMENTAcute Rheumatic fever • Inj. Benzathine Penicillin 12 lac units i.m single dose • OR Erythromycin 40mg/kg/day in 2-4 divided doses for 10days • Aspirin 100mg/kg/day in 4-5 divided doses for 3-4 wks, dose is gradually tapered depending upon ESR & CRP levels.
Treatment of Rheumatic Carditis • Without Failure • Same as ARF • If no response to aspirin ,start Corticosteroids • With Failure/severe carditis • Prednisone 1-2mg/kg/day for minimum of 2 wks & then tapered for next 2 wks
Aspirin is started during the tapering course of Corticosteroids and is continued for 4 wks or until there is sufficient clinical &laboratory evidence of reduced rheumatic activity • Aspirin for minimum 12 wks • It is given to reduce the rebound activity after stopping of steroids. • 5% of patients of ARF continue to have rheumatic activity for >6mths
SEVERE CASES • Anti failure therapy • SURGICAL THERAPY • Mitral valve repair • Mitral valve replacement
Prevention of RF PRIMODIAL PREVENTION • Involves measures to prevent the occurrence of a GABHS sore throat • Clean & Healthy environment. • Mass chemoprophylaxis can work in some high risk situations • Vaccines are in experimental phase • Not feasible in all situations
Primary prophylaxis • Benzathine penicillin G <27kg 0.6 MU IM Once >27kg 1.2 MU • PenicillinV Children 250mg bd/tid PO 10days Adults 500mg bd/tid • Penicillin allergy Erythromycin 250mg qid PO 10days Azithromycin 500mg PO 1 day 250mg OD 4 days • Others – nafcillin, ampicillin, amoxycillin, clindamycin, cephalexin
SECONDARY PREVENTION • Involves prevention of streptococcal sore throat in patients with previous episodes of RF & thereby prevent recurrent cardiac damage • RF is a recurrent disease • Recurrence per infection 40-60% • Permanent cardiac damage increases with Recurrences
Secondary prophylaxis Benzathine penicillin G 1.2MU IM Penicillin V 250mg BD PO Sulfadiazine <27kg 500mg OD PO >27kg 1000mg Penicillin/ sulfa allergy Erythromycin 250mg BD PO