Download

1 / 75
750 likes | 816 Views
Physiology of the Cerebrospinal Fluid and Intracranial Pressure. Chapter 10 Presentation: S. Bahram Seif, Resident of Neurosurgery Isfahan University of Medical Sciences. Protective and Homeostatic Systems of the CNS. Skull Bones ( physical protection )

E N D
Physiology of theCerebrospinal FluidandIntracranial Pressure Chapter 10 Presentation: S. Bahram Seif, Resident of Neurosurgery Isfahan University of Medical Sciences
Protective and Homeostatic Systems of the CNS • Skull Bones (physical protection) • CSF(hydraulic shock absorption) • Continuous Turnover of Extracellular Fluid (substrate supply and cellular homeostasis) • BBB
Elevated ICP • Congenital lesions • Neoplasms • Metabolic syndromes • Infectious syndromes • Infarction • Hemorrhage • Trauma
HISTORICAL CONSIDERATIONS • Galen • Hippocrates • Early Egyptian physicians Removing Pieces Of Skull
19th Century • Alexander Monro • George Kellie Monro-Kellie Doctrine
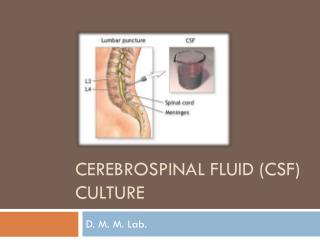
Lumbar Puncture • 1911 • Quincke • 1951 continuously ICP monitoring • Lundberg
NORMAL INTRACRANIAL PRESSURE • Upper limit of normal ICP: 15 mmHg • Usual range is 5 to 10 mmHg • Coughing or Sneezing: 30 to 50 mmHg
ICP Evaluation • Intraventricular • Intraparenchymal • Subdural • Epidural
CSF Pulsatility • Associated with Cardiac andRespiratoryactivity • Changes in these pulsatile components can be one of the earliest signs
Cardiac Component • Left ventricular contraction • Peripheral arterial pulse • Choroid plexus and pial arteries • High-compliance venous blood vessels
Respiratory Component • Generated by pressure changes in the thoracic and abdominal cavities
Percussion wave (WI), the most constant, Pulsations in large intracranial arteries. • Tidal wave (W2), brain elastance. • Dicrotic wave (W3), dicrotic notch in the arterial.
ICP is synonymous with CSF Pressure
Atmospheric pressure • Hydrostatic pressure • Filling pressure
As volume is added there are two principal routes for compensation
Distention of the spinal dura mater • Displacement of CSF and blood
ICP depends on the total volume inside the skull
Intracranial Space: 1500-mL • 87%: the Brain • 9%: CSF (ventricles, cisterns, and subarachnoid space) • 4%: blood
CSF • Compartmental • Extracellular space 164.5 mL
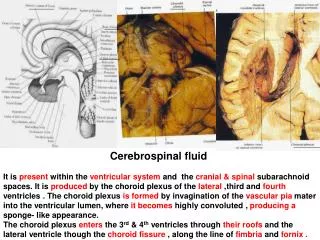
CSF Production • Choroid plexuses • Ventricular ependyma
Choroid Plexuses • Invaginations of the pia mater into the ventricular cavities Roofs of the third and fourth ventricles Walls of the lateral ventricles
Energy-dependent secretion and reabsorption processes • 0.35 to 0.37 mL/min
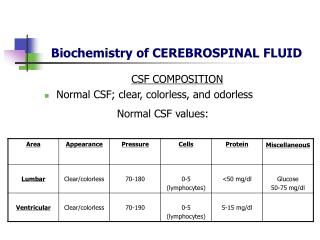
Higher sodium, chloride, and magnesium • Lower potassium, calcium, urea, and glucose • Similar osmolality
Peak Production Rates Late evening Early morning
CSF Drainage • Dural Venous System Even in CSF pressures of less than 5 mm Hg
NPH • Ventricular enlargement • Absence of elevated ICP
Gait disturbance • Dementia • Incontinence
Symptoms and Signs of ElevatedIntracranial Pressure • Depends greatly on the nature and anatomic location of the underlying pathologic condition • Headache, vomiting and papilledema.
Cranial nerve palsies may arise as a result of pressure on brainstem nuclei (particularly abducens palsies)
Papilledema • Reliable • Objective • Good specificity • Sensitivity: observer dependent
Vital Sign Changes • Cushing response: Arterial Hypertensionand Bradycardia
Abnormal Respiration • Cheyne-Stokes: diencephalic region • Sustained hyperventilation: midbrain and upper pons • Slow respiration: Midpontine • Ataxic respirations: pontomedullary lesions • Rapid shallow breathing: upper medullary lesions
Herniation Syndromes • Most serious complication of raised lCP
Central Syndrome • Progressive dysfunction of structures in a rostral to caudal direction • 1st Diencephalic Structures: Change in behavior or even loss of consciousness, Cheyne-Stokes respiration • Pupils :small, with a poor reactivity • Contralateral hemiparesis • Pupils fall into a midline fixed position
Uncal Syndrome • Unilaterally dilated and poorly reactive pupil • External oculomotor ophthalmoplegia • Ipsilateral hemiparesis: pressure on the contralateral cerebral peduncle on the edge of the tentorium cerebelli