Women's Roles in Malaria Prevention: A Study in Mali Villages
This study explores the pivotal role of women in managing malaria transmission in Malian villages, highlighting the need for community-wide involvement and education. Women, especially elder women, emerge as key players in combating malaria through preventive measures and care for at-risk children. The results underscore the importance of holistic approaches and community engagement in malaria eradication efforts.

Women's Roles in Malaria Prevention: A Study in Mali Villages
E N D
Presentation Transcript
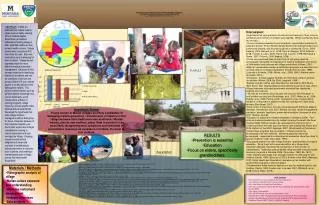
Hypothesis Tested: Young women in Malian villages are likely candidates for managing malaria prevention / transmission of malaria in their village because their traditional roles as African / Muslim women, also as new mothers, place them in position to be most likely recognizing early symptoms and interested in preventative measures as caretakers of infants, the most at-risk children. • With Gratitude: • My husband for constant support and encouragement • Prof. Florence Dunkel for her role as a muse • Prof Ada Giusti for insight and translation • The time and honesty of those interviewed; including the Queen Mother, Sidy Ba, and Belko • The village of Sanambele • The fall 08’ “Health, Poverty and Agriculture” class • Funding from: MSU Undergraduate Scholars Program (P. Powers-Peprah); Montana Ag Experiment Station #161 (F. Dunkel); USDA Higher Education Challenge Grant # 2007-38411-18609 (F. Dunkel). • RESULTS • Prevention is essential • Education • Focus on elders, specifically grandmothers • Materials / Methods • Videographic analysis of village • Malian culture exposure and understanding • Interview instrument development • In-depth interviews • Data-analysis Introductory Study of Women’s Roles in Holistic Management of Malaria in an Isolated, Traditional Subsistence Farming Village in Mali Author: Pauline E. Powers-Peprah; Mentor: Florence V. Dunkel Departments: Cell Biology and Neuroscience; Plant Sciences and Plant Pathology ABSTRACT: In Mali, an estimated two million malaria cases occur annually causing 50% of children deaths. Sanambele, an isolated subsistence farming village in Mali, identified malaria as their primary health concern. Village women were concerned 40% more than the men. Bed nets / medication were challenging for them to obtain. Village women expressed need for more effective malaria prevention / management. Because of their stronger response in identifying malaria as a problem and role as caretakers of at-most-risk group (children 0-5 yrs), women appear to be key players in the fight against malaria. This project explored factors such as general malaria knowledge and current treatments, social infrastructure, efficacy of existing programs, village hierarchy, women specific roles, spiritual and personal beliefs. We tested the hypothesis that older village children/ teenagers would be ideal group for focus. However, because of their respected position, we found elder women are stronger candidates for training in malaria prevention and care amongst the village. Ongoing research entails ethical obligations of developed countries in contributing to malaria prevention in resource-poor countries, and creating a manual based upon a village survey, that may benefit Sanambele. • Discussion: • Hypothesis that young women should be focus because of their roles as caretakers and mothers ofchildren was rejected. Whole community must be involved. • Current malaria prevention focus is bednets / preventative medicine for pregnant women. Peer-refereed literature/interviews indicate malaria is a community disease, and must be fought as a community (Tiono, 2008; Bellamy, 2004; Bennett, et al., 2008; Bove & Valeggia, 2009; Editorial, 2008; Francke & Lalou, 2009; Fraser-Hurt & Lyimo, 1998; Mathanga & Bowie, 2007; Pincock, 2008; Wakabi, 2008). • Those more removed than mothers from at risk group must be encouraged / educated on importance of malaria eradication,connection of child deaths and sickness with village productivity (Killeen, 2007). • Bed net / preventative medicine distribution programs are beneficial, but not final solution to malaria eradication (Fraser-Hurt & Lyimo, 1998), (Launiala & Kulmala, 2006) (Muller, et al., 2008) (MALI: Malaria cases decrease, 2004). • Interviews / articles suggest bednets are most likely used for parents, not children (Muller, 2008; Ba 2008; Lampietti, 1999). • Bednet program neither well advertised nor adhered to (IRIN Africa-West Africa- Mali- Beating Malaria achievable this year gov't says, 2007). Village interviews indicated government-promised free medicines / bednets did not arrive. • Women do not attend clinics usually until second / third trimester, or until children are very sick (Brentlinger, et al., 2007; Muller, et al., 2008; Rosato, et al., 2006; Parise, 2003). Complete course of preventative medicine is important in addition to bed net coverage for health baby delivery (Brentlinger, 2007) • Other forms of prevention must be incorporated with Roll Back Malaria initiatives (Hommerich et al, 2007, Malaria Journal), larvae management, sanitation, bednets, repellants, preventative medicine (Hommerich et al, 2007, Malaria Journal). • Education is essential for malaria eradication )(Bellamy, 2004). Few promote breaking transmission by bednet covering those with the fever (Dunkel 2008). Mothers need to be reminded of moments to act in covering children with nets and how fast to seek medical aid (Boller et al, 2003, Bulletin of the WHO; Adeneye, 2007, World Health & Population). • Government programs are not reliable.. Villagers need to be encouraged to be self-sufficient. Women especially need to be encouraged / supported in entrepreneurial endeavors since they likely to pay for medicine / bed nets (Castle, 1993). • Pay special attention to older village mothers / grandmothers in malaria education. Since they hold a revered position as a village elder, education attempts must keep the specialness of their position in consideration. Traditional spiritual beliefs influence older women’s health decisions (Launiala & Kulmala, 2006; Omorodion, 1993; Bâ, 1972). • Older mothers wait longer than younger mothers to seek help for sick children (Castle, 1993) (Boller et al, 2003, Bulletin of the WHO; Adeneye, 2007, World Health and Population), and were not as familiar with government programs or policy changes. • Grandmothers make financial decisions to pay for medical care for sick children (Castle, 1993; Dunkel et al. in review, 2007; Whitworth, et al., 2008; Anya & Raine, 2008). SURVEY INSTRUMENT See attached LITERATURE CITED Anya, I., & Raine, R. (2008). Strengthening clinical and research ethics in Nigeria--an agenda for change. Lancet , 1594-7. Bâ, A. H. (1972).Aspects de la civilisation africaine. Présence Africaine. Bellamy, C. (2004). Globalization and Infectious Diseases in Women. Emerging Infectious Diseases , 2022-2024. Bennett, S., Adam, T. A., Zarowsky, C., Tangcharoensathien, V., Ranson, K., Evans, T., et al. (2008). From Mexico to Mali: progress in health policy and systems research. Lancet , 1571-1578. Bove, R., & Valeggia, C. (2009). Polygyny and women's health in sub-Saharan Africa. Social Science Medicine , 21-9. Brentlinger, P. E., Dgedge, M., Correia, M. A., Rojas, A. J., Saute, F., Gimbell-Sherr, K. H., et al. (2007). Intermitten preventive treatment of malaria during pregnancy in central Mozambique. Bulletin of the World Health Organization , 873-879. Editorial. (2008). The Bamako call to action: research for health. Lancet , 1855. Francke, A., & Lalou, R. (2009). Health Seeking Behaviour for childhood malaria: household dynamics in rural Senegal. Journal of Biosocial Scienceq , 1-19. Fraser-Hurt, N., & Lyimo, E. (1998). Insecticide treated nets and treatment service: a trial using public and private sector channels in rural United Republic of Tanzania. Bull World health Organ, 76, 607-615. Launiala, A., & Kulmala, T. (2006). The importance of understanding the local context: Women's perceptions and knowledge concerning malaria in pregnancy in rural Malawi. Acta Tropica , 111-117. MALI: Malaria cases decrease. (2004, March). Retrieved September 27, 2008, from Science in Africa: http://www.scienceinafrica.co.za/2004/march/malaria.htm Mathanga, D., & Bowie, C. (2007). Malaria control in Malawi: are the poor being served? International Journal for Equity in Health, 6 (22). Muller, O., De Allegri, M., Becher, H., Tiendrebogo, J., Beiersmann, C., Ye, M., et al. (2008). Distribution Systems of Insecticide-Treated Bed Nets for Malaria Control in Rural Burkina Faso: Cluster-Randomized Controlled Trial. PLoS Hub for Clinical Trials . Omorodion, F. (1993). The socio-cultural context of health behaviour among Esan communities, Edo State, Nigeria. Health Transition Review , 125-135. Pincock, S. (2008). Ogobara Doumbo: building capacity for malaria research in Africa. Lancet , 1537. Rosato, M., Mwansambo, C. W., Kazembe, P. N., Phiri, T., Soko, Q. S., Lewycka, S., et al. (2006). Women's groups' perceptions of maternal health issues in rural Malawi. The Lancet , 1180-1188. Wakabi, W. (2008). Research collaboration boosts women's health in Ethiopia. Lancet , 1534. Whitworth, J. A., Kokwaro, G., Kinyanjui, S., Snewin, V. A., Tanner, M., Walport, M., et al. (2008). Strengthening capacity for health research in Africa. Lancet , 1590-3. • General Knowledge Questions: • Have you had Malaria? • What was it like? • Who took care of you? • Were you given medicine? • Where did it come from? • What other treatments are there for Malaria? • What do you know about Malaria? • Bednet Questions: • Did you use bednets? • Do you know how to use bednets? • Are bednets practical for use in your village as malaria management? • Who has bednets in your community? • How are they distributed? • How many people can use one bed net? Is this reasonable? • Would bednets fully manage malaria? • Are there other factors necessary in management? • DDT Questions: • Are pesticides used in your village? • Do you think if your village was able to have access to a pesticide like DDT, which is extremely fatal to bugs, but also very poisonous and toxic to humans, and does not break down in the water, but stays around, that they would still use it? • Do you think they would use it for their plants even if it were only intended for mosquito control, to be used one time only? • Do you think it would go on the black market? • Management Questions: • What do people in your village do when there are malaria outbreaks? • Are there agencies that work in your village to help with malaria? • What would you like to see for management of malaria? • Do you think the government should help? • Do you think countries like America should help? • If so, how should they help? • Do you think it’s reasonable that if malaria could be controlled on the village level, to believe these methods could be used on a larger scale, to control malaria at the country level? • If somebody outside of the village were to come in to try to help implement a new method of malaria control, what would your advice to do so be? • Part of the challenge of malaria is the mutation rate of the parasite, and resistance to medicine. Do you think villagers understand the importance of taking the complete dose of medicine? • What factors prevent this from happening? • DDT Questions: • Are pesticides used in your village? • Do you think if your village was able to have access to a pesticide like DDT, which is extremely fatal to bugs, but also very poisonous and toxic to humans, and does not break down in the water, but stays around, that they would still use it? • Do you think they would use it for their plants even if it were only intended for mosquito control, to be used one time only? • Do you think it would go on the black market? • Social Infrastructure: • Do you see differences in who gets malaria and which children die from it based upon social class? • Do you see Malaria as a community disease, or individual disease? • Are men involved in managing malaria? Should they be? What about women? What about teenagers? • Who in your village primarily cares for the children under 5? • When somebody comes down with malarial fever, how are they handled? • Who cares for them? • Are there taboos associated with malaria and people who have it? • Women Specific Questions: • How do women in your village raise funds? • Are there any cottage industries? • Who manages the money that the women raise? • What are traditions in your village for women? • Are these changing? • Should they be preserved? • Do the wives live with their mother-in-laws? • Who makes the decisions in the household regarding health care? • Who makes the financial decisions regarding healthcare for children? • What does the village religion demonstrate to you about women? • How old are the women when they get married? • What is the ceremony for marriage? • Are girls educated? • When do they go to school or what prevents them from attending? • Are certain ages associated with certain responsibilities? • Village Questions: • Who are the leaders in your village? • How are they determined? • How does it affect your village when there is a malaria outbreak? • Is it necessary to work through a “representative” of the village if a non-villager wanted to help the village? • Is your village’s ability to provide and care for itself impacted by malaria? • How? • In the village, is there a communal pot, where all members are able to benefit from it? How are such things as crop failures handled? • Are there people who are considered “lazy”? • How are they treated? • Is there a free clinic nearby? • Would it help if there was one? • Does it help if there is one? • How hard is it to get there? • Is there corruption? • What has already been attempted in your village to control Malaria? • Was it effective? • What made it so? • Do people in your village accept malaria as a “fact of life” to the point where living without it is almost unimaginable? • How does your village get its water? • Who is responsible for providing water to the household? • What are the main uses of water in your village? (I.E. is it relied upon for agriculture, building bricks, etc)? • Do you have a map of your village? • Who are the key players in your village? • Who does the village turn to when there is a community problem? • What are the main staples of food in your community? • Where does this food come from? • Who prepares it? • Is there freedom of speech in your village? • Do they have influence in how an epidemic would be handled? • Who would you ask for help from if your village was undergoing an epidemic? • Spiritual/Religious Questions: • What rituals does your village participate in? • Are there specific ceremonies? • Rites of passage? • What is the primary religion in your village? • Does that religion affect the management of malaria/illness? • Do villagers believe in witchcraft? (If yes, ask following questions): • To what extent does this belief influence healthcare? • Have you ever seen witchcraft rituals performed? • Are there particular people who would perform the rituals, or can anybody perform them? • What are symptoms of a curse? • How do you know if someone has been cursed? • For what reasons are people cursed? • How does a villager protect themselves from, and/or counteract a curse? • Are there certain groups, such as women, who are cursed more often? • If yes, why do you think this is so? • Personal Belief Questions: • What would you identify as the top three major health concerns in your country, not including AIDS? (This question was asked first, but categorized as a personal belief question.) • How do you define poverty? • How does poverty affect management of malaria? • Have you heard or seen other methods of managing malaria that were effective? • What are the reasons programs have not been effective in your opinion? • Do you think it is more important when there is a malaria outbreak to get it under control as quickly as possible, even if that means missing an opportunity to discover a long term solution? Or is it important to use that outbreak as an opportunity to experiment with solutions and possibly discover a working method that may not control malaria as immediately, but would be more effective long term? • Do you believe other countries that have more financial resources, such as European and American, are obligated to help a country like Africa control malaria? • Do you think ex-patriots, people who have left your country, would come home if conditions improved? • What would have to improve? • How long do you think it would take? • What would you like Americans to know about Malaria management? • Do you have questions for me? Discussion: The focus of prevention of malaria seems to be on bednets and preventative medicine for pregnant women. However, it is evident from the articles reviewed, as well as the interviews conducted that malaria is a community disease, and must be fought as a community (Alfred B Tiono, 2008), (Bellamy, 2004), (Bennett, et al., 2008), (Bove & Valeggia, 2009), (Editorial, 2008), (Francke & Lalou, 2009), (Fraser-Hurt & Lyimo, 1998), (Mathanga & Bowie, 2007), (Pincock, 2008), (Wakabi, 2008). The original hypothesis that young women should be the focus because of their roles as caretakers and mothers of children was rejected based upon the interviews. The whole community must be involved. Those who are somewhat more removed than the mothers from the most at risk group must be encouraged and educated upon the importance of malaria eradication and the connection of child deaths and sickness with the overall productivity of the village (Killeen, 2007). The bed net and preventative medicine distribution programs seem to be beneficial, yet are not a final solution to eradication of malaria (Fraser-Hurt & Lyimo, 1998), (Launiala & Kulmala, 2006) (Muller, et al., 2008) (MALI: Malaria cases decrease, 2004). Several challenges within the program exist. First of all, as revealed through an interview with Professor SidyBa, as well as article review, the bednets are most likely to be used for the parents, not the children (Muller, 2008) (Lampietti, 1999). Secondly, the program appears to be neither well advertised nor adhered to. As stated previously, Mali initiated the program in 2007, yet there was only one article that discussed it in the article review and search (IRIN Africa-West Africa- Mali- Beating Malaria achievable this year gov't says, 2007). Additionally, the midwife in Sanambele did not seem to have awareness of the program since she stated she desperately needed medicine and bednets for the area’s children during this year’s rainy season. Another important factor is that in other countries where similar programs have been initiated, women do not attend clinics usually until their second or third trimester, or until children are very sick (Brentlinger, et al., 2007) (Muller, et al., 2008) (Rosato, et al., 2006). This means that women are not receiving bednets during their first trimester, where medicine is deleterious. Women also are inconsistently returning to the clinics for their second and third rounds of preventative medicine. The women who do return were found to have concerns regarding the effect of preventative medicine on their fetus (Parise, 2003). The complete course of preventative medicine was shown to be important in addition to bed net coverage for delivery of healthy babies (Brentlinger, 2007) Other forms of prevention must be incorporated with Roll Back Malaria initiatives. Prevention has been stressed as most important factor by articles & interviews (Hommerich et al, 2007, Malaria Journal). Forms of prevention include larvae management, sanitation, bednets, repellants, and preventative medicine in the sense of neonatal care although caution should be used since “a substantial increase in the proportion of resistant parasites has been observed within weeks after preventive SP treatment… Meanwhile alternative options to SP in intermittent prevention medicine should urgently be evaluated” (Hommerich et al, 2007, Malaria Journal). Education is essential for malaria eradication. It is very important to continue reminding the villagers of what they have already learned, and for outside groups to continue to reach the whole village as a community with new education (Bellamy, 2004). Mothers need to be reminded of key moments to act in covering children with nets; older mothers were identified as waiting longer than younger mothers in seeking medical help for sick children (Boller et al, 2003, Bulletin of the WHO), and were not as familiar with government programs or policy changes (Adeneye, 2007, World Health & Population). As discussed previously, government programs are not reliable, and it is important for the villagers not to be waiting for them to help. All those interviewed identified government management and allocation of resources as an area of improvement. The villagers need to be encouraged and provided with self-sufficiency. Women especially need to be encouraged and supported in their entrepreneurial endeavors since they are the ones who allocate their resources and would be likely to pay for medicine and bed nets (Castle, 1993). Special attention should be paid to older village mothers and grandmothers regarding malaria education. Since they hold a revered position as a village elder, education attempts must keep the specialness of their position in consideration. Additionally, it is the grandmothers who are likely to be interacting with the healthy children since the mothers would be going about daily responsibilities in the village and fields. Traditional spiritual beliefs are more likely to influence older mothers and grandmothers decisions in health care for the children as well (Launiala & Kulmala, 2006) (Omorodion, 1993) (Bâ, 1972). Older mothers were identified as waiting longer than younger mothers in seeking medical help for sick children (Castle, 1993) (Boller et al, 2003, Bulletin of the WHO) up to “24-48 hours or more, relying on their wealth of experience in child care.” (Adeneye, 2007, World Health and Population), and were not as familiar with government programs or policy changes (Adeneye, 2007, World Health & Population). In households where the mothers and grandmothers are living together, it may be the grandmother who is making the financial decisions to pay for medical care for sick children (Castle, 1993). They may also choose traditional medicine, although strengths, timing of administration, as well as timing of harvesting are all areas that need further investigation (Dunkel et al. in review, 2007) (Whitworth, et al., 2008) (Anya & Raine, 2008).