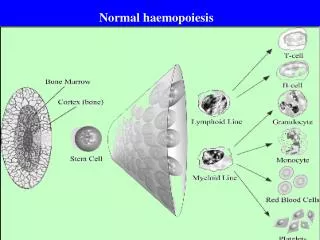
Normal haemopoiesis
430 likes | 576 Views
Normal haemopoiesis. ABNORMALITIES IN THE HEMOPOIETIC SYSTEM. CAN LEAD TO HEMOGLOBINOPATHIES HEMOPHILIA DEFECTS IN HEMOSTASIS/THROMBOSIS HEMATOLOGICAL MALIGNANCY. MUTATIONS AND DNA. VARIOUS TYPES OF MUTATIONS CAN OCCUR LEADING TO DISEASE PHENOTYPE POINT MUTATIONS INSERTIONS OR DELETIONS

Normal haemopoiesis
E N D
Presentation Transcript
ABNORMALITIES IN THE HEMOPOIETIC SYSTEM • CAN LEAD TO • HEMOGLOBINOPATHIES • HEMOPHILIA • DEFECTS IN HEMOSTASIS/THROMBOSIS • HEMATOLOGICAL MALIGNANCY
MUTATIONS AND DNA • VARIOUS TYPES OF MUTATIONS CAN OCCUR LEADING TO DISEASE PHENOTYPE • POINT MUTATIONS • INSERTIONS OR DELETIONS • TRANSLOCATIONS • COMPLEX CHROMOSOMAL REARRANGEMENTS
VARIABILITY IN GENETIC DISEASES • ONE DISEASE, ONE GENE, ONE MUTATION • ONE DISEASE, ONE GENE, MANY MUTATIONS • ONE DISEASE, MORE THAN ONE GENE, MANY • MUTATIONS
HAEMOPHILIA X LINKED RECESSIVE DISORDER HAEMOPHILIA A – MUTATIONS IN FACTOR VIII GENE HAEMOPHILIA B – MUTATIONS IN FACTOR IX GENE SIMPLE AND COMPLICATED MUTATIONS THE FLIP TIP MUTATION
E1 E22 E23 E26 F8A F8B A CEN TEL B TEL E1 E22 E23 E26 CEN F8A C E22 E1 E23 E26 TEL CEN INVERSION 22 FIGURE 4 THE IVS 22 MUTATION IN HAEMOPHILIA A.
Genetic factors and deep vein thrombosis • FACTOR V LEIDEN MUTATION • PROTHROMBIN MUTATION • ? OTHER FACTORS IN THE PROTEIN C PATHWAY • FVL LEADS TO SIGNIFICANT INCREASE IN RISK OF DVT, PARTICULARLY IN ASSOCIATION WITH OTHER ENVIRONMENTAL FACTORS EG OCP
HOW DOES A CELL BECOME TUMORIGENIC? • THREE PROCESSES ARE INVOLVED • IMMORTALISATION • TRANSFORMATION • METASTASIS
IMMORTALISATION • PROCESS BY WHICH THE CELLS ARE INDUCED TO GROW INDEFINITELY
TRANSFORMATION • CELLS ARE NOT CONSTRAINED IN TERMS OF GROWTH CHARACTERISTICS AND TEND TO BECOME FACTOR INDEPENDENT
METASTASIS • CANCER CELLS GAIN THE ABILITY TO INVADE NORMAL TISSUE AND ESTABLISH OTHER FOCI OF MALIGNANCY
WHAT CAUSES CELL TRANSFORMATION? • ENVIRONMENTAL • CARCINOGENS(INITIATORS AND PROMOTERS) • GENETIC • SOMATIC MUTATIONS • MENDELIAN INHERITANCE
ONCOGENES • NORMAL CELLULAR COUNTERPARTS(PROTO-ONCOGENES) • MUTATION/ACTIVATION LEADS TO TUMOR FORMATION • HUNDREDS OF ONCOGENES IDENTIFIED • GAIN OF FUNCTION
Tumour suppressor genes • Originally known as recessive oncogenes • Need to have both copies of the gene affected to promote a malignant phenotype • Knudsons 2 hit hypothesis • First mutation makes cells susceptiple to development of cancer • 2nd hit leads to a malignant phenotype
TRANSLOCATIONS AND CANCER • SEEMS PARTICULARLY RELEVANT IN HEMATOLOGICAL MALIGNANCIES • CHRONIC MYELOID LEUKEMIA • ACUTE PROMYELOCYTIC LEUKEMIA • BURKITTS LYMPHOMA • NON HODGKINS LYMPHOMA
Leukaemia, the current hypothesis • Defect in maturation of white blood cells • May involve a block in differentiation and/or a block in apoptosis • Acquired genetic defect • Initiating events unclear • Transformation events involve acquired genetic changes • Chromosomal translocation implicated in many forms of leukaemia
Chronic Myeloid Leukaemia • Malignancy of the haemopoietic system • Transformation of the pluripotent stem cell • 9;22 translocation giving rise to the Philadelphia (Ph’) chromosome • Creation of a leukaemia specific mRNA (BCR-ABL) • Resistance to apoptosis, abnormal signalling and adhesion • Molecular diagnostics • Molecular and cellular therapeutics
Cytogenetic Abnormality of CML:The Ph Chromosome 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 x Y
The Ph Chromosome: t(9;22) Translocation 9 9 q+ 22 Ph ( or 22q-) bcr bcr-abl abl FUSION PROTEINWITH TYROSINEKINASE ACTIVITY
Prevalence of the Ph Chromosome in Haematological Malignancies Leukaemia % of Ph+ Patients CML 95 ALL (Adult) 15–30 ALL (Paediatric) 5 AML 2 Faderl S et al. Oncology (Huntingt). 1999;13:169-184.
bcr-abl Gene and Fusion Protein Tyrosine Kinases Chromosome 22 Chromosome 9 c-bcr 2-11 1 c-abl 2-11 p210Bcr-Abl 2-11 p185Bcr-Abl Exons Introns CML Breakpoints ALL Breakpoints Adapted from Melo JV. Blood. 1996;88:2375-2384.
NON HODGKINS LYMPHOMA • B CELL FOLLICULAR LYMPHOMA • t(14;18)(q21;q14) • BCL 2 AND IMMUNOGLOBULIN GENES INVOLVED • DYSREGULATION OF BCL 2 • FAILURE OF APOPTOSIS
Detecting Cancer – different markers for different diseases?
Cancer Molecular Diagnostics – discriminating cancers at the gene level
How Cancer Molecular Diagnostics? • Chromosome analysis • Gene analysis • Gene expression analysis • Protein analysis • Gene chip analysis
Leukaemia diagnostics • Morphology • Cytogenetics • Fluorescent In Situ Hybridisation (FISH) • Immunophenotyping • PCR of chromosomal translocations
New developments in Cancer Molecular Diagnostics The Gene Chip
MOLECULAR MEDICINE • A new approach to medicine • New Diagnostics • New Therapeutics • A number of agents now in clinical trials • Molecular medicine will help identify new targets and permit rational drug development