Red cell disorders
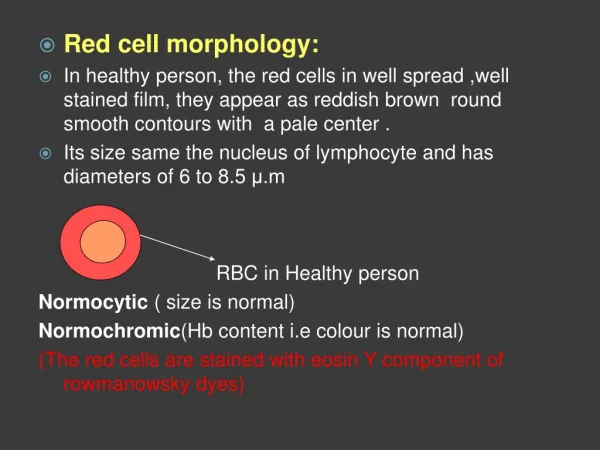
Red cell disorders. Disorders of red cells can result in anemia or, less commonly, polycythemia (an increase in red cells also known as erythrocytosis ).

Red cell disorders
E N D
Presentation Transcript
Disorders of red cells can result in anemia or, less commonly, polycythemia (an increase in red cells also known as erythrocytosis). Anemia is defined as a reduction in the oxygen-transporting capacity of blood, which usually stems from a decrease in the red cell mass to subnormal levels Anemia can result from bleeding, increased red cell destruction, or decreased red cell production. These mechanisms serve as one basis for classifying anemias RED CELL DISORDERS
Pathology of Anemias • Causes: • Blood loss (hemorrhage) • Increased red cell destruction (hemolysis) • Decreased red cell production • Morphology: • Microcytic (iron deficiency, thalassemia) • Macrocytic (folate or vitamin B12 deficiency) • Normocytic but with abnormal shapes (hereditary spherocytosis, sickle cell disease)
Clinical Manifestations : • Acute: shortness of breath, organ failure, shock • Chronic • Pallor, fatigue, lassitude • With hemolysis: jaundice and gallstones • With ineffective erythropoiesis: iron overload, heart and endocrine failure • If severe and congenital: growth retardation, bone deformities due to reactive marrow hyperplasia
ANEMIA OF BLOOD LOSS • acute blood loss : • If exceeding 20% of blood volume hypovolemic shock rather than anemia. • If the patient survives, hemodilution begins at once and achieves its full effect within 2 to 3 days; only then is the full extent of the red cell loss revealed. • The anemia is normocytic and normochromic. • Recovery from blood loss anemia is enhanced by a compensatory rise in the erythropoietin level, which stimulates increased red cell production and reticulocytosis within a period of 5 to 7 days. • With chronic blood loss: iron stores are gradually depletedIron deficiency anemia • Iron is essential for hemoglobin synthesis and erythropoiesis, and its deficiency leads to a chronic anemia of underproduction.
HEMOLYTIC ANEMIAS • Normal red cells have a life span of about 120 days. • Anemias caused by accelerated red cell destruction are termed hemolytic anemias. • Destruction can be from either: 1- intrinsic (intracorpuscular) red cell defects, which are usually inherited 2- extrinsic (extracorpuscular) factors, which are usually acquired
Features shared by all hemolytic anemias • a decreased red cell life span • a compensatory increase in erythropoiesis • retention of the products of degraded red cells (including iron) by the body. • associated with erythroid hyperplasia in the marrow and increased numbers of reticulocytes in the peripheral blood. • In severe hemolytic anemias, extramedullaryhematopoiesis may appear in the liver, spleen, and lymph nodes
Thalassemia • are inherited disorders caused by mutations that decrease the synthesis of α- or β-globin chains. • As a result, there is a deficiency of Hb and additional red cell changes due to the relative excess of the unaffected globin chain • particularly common among populations in Mediterranean, African, and Asian regions • adult hemoglobin, or HbA, is a tetramer composed of two α chains and two β chains. The α chains are encoded by two α-globin genes, which lie in tandem on chromosome 11, while the β chains are encoded by a single β-globin gene located on chromosome 16
The anatomic changes in β-thalassemia major - hyperplasia of erythroid progenitors expanded erythropoietic marrow may completely fill the intramedullary space of the skeleton: • skeletal deformities. • splenomegaly,hepatomegaly, and lymphadenopathy. • growth retardation • Cachexia • Hemosiderosis (iron overload)
ANEMIAS OF DIMINISHED ERYTHROPOIESIS • includes anemias that are caused by : 1- inadequate dietary supply of nutrients: e.g. iron, folic acid, and vitamin B12. 2- anemias associated with bone marrow failure (aplastic anemia) 3- anemia of chronic disease (systemic inflammation) 4- bone marrow infiltration by tumor or inflammatory cells (myelophthisic anemia).
Iron Deficiency Anemia • the most frequent cause of anemia is iron deficiency.. • developed countries 10% of people • developing countries 25% to 50% • Morphology: • red cells are microcytic and hypochromic. • low serum ferritin and iron levels, low transferrin saturation • increased total iron-binding capacity • response to iron therapy. • For unclear reasons, the platelet count often is elevated. Erythropoietin levels are increased
PATHOGENESIS: • Chronic blood loss is the most important cause of iron deficiency anemia in the Western world - (e.g., peptic ulcers, colonic cancer, hemorrhoids) and the female genital tract • In the developing world, low intake is the most common causes of iron deficiency. • Increased demands not met by normal dietary intake occur worldwide during pregnancy and infancy. • Malabsorption can occur with celiac disease or after gastrectomy
Polycythemia= erythrocytosis • an increase in red cells per unit volume of peripheral blood, usually in association with an increase in hemoglobin concentration. • Polycythemia may be absolute (defined as an increase in total red cell mass) or relative. Relative polycythemia results from dehydration, such as occurs with water deprivation, prolonged vomiting, diarrhea, or the excessive use of diuretics. • Absolute polycythemia is described as primary when the increased red cell mass results from an autonomous proliferation of erythroid progenitors, and secondary when the excessive proliferation stems from elevated levels of erythropoietin. Primary polycythemia (polycythemiavera) is a clonal, neoplasticmyeloproliferative disorder considered later in this chapter. • The increases in erythropoietin that cause secondary forms of absolute polycythemia have a variety of causes