Download
1 / 15
330 likes | 2.21k Views
REVIEW OF CASES. In a 1yr retrospective study in our hospital( Jan2009

E N D
1. CEREBRAL VENOUS THROMBOSIS IN PREGNANCY-AN EMERGING CATASTROPHY ?? Dr. SUKANYA .M. K
BANGALORE BAPTIST HOSPITAL
UNDER GUIDANCE OF DR. PADMAJA
HOD, DEPARTMENT OF OBG
BANGALORE BAPTIST HOSPITAL
2. REVIEW OF CASES In a 1yr retrospective study in our hospital( Jan2009 � Dec 2009), out of 7 cases of stroke in pregnancy 5 cases of cerebral venous thrombosis were reported
i.e 71% of stokes in pregnancy.
2 of the patients were antenatal (40%) and 3 of them were postnatal (60%).
80% of patients presented with seizures , 80%with headache .
80% recovered completely with early diagnosis and rapid management and 20% was the mortality.
Here we are presenting a review of these cases.
3. primigravida, 26yrs,17wks
Chronic hypertension since 7wks
h/o headache,blurring of vision -1 week
Fundoscopy-papilledema
ECHO- normal
MRI- normal
MRV � hypoplastic old thrombosed and recanalised left transverse sinus- focal thrombosis
Rx � Anticoagulants , referred to NIMHANS for second opinion G3P2L2 ,28yrs,33wks
h/o OCP use
h/o of headache , blurring of vision � 1day, h/o convulsions (GTCS) >10 episodes with loss of consciousness, h/o weakness of rt side of body with deviation of mouth to left
Fundoscopy -normal
MRI- recent small infarct of left posterior lobe venous infarct
MRV- thrombosis of rt transverse sinus.
Had normal vaginal delivery after 2days
4. 3 postnatal cases were reported.
Age of the patients ranged 21-27 yr
Presented after 13-15 days of delivery
All the 3 patients presented with headache, vomiting and seizures. 1 patient was unconscious and was declared brain dead.MRI & MRV showed thrombosis of straight sinus with infarct in the thalamic and basal ganglia region. Other 2 patients had thrombosis of transverse and superior sagittal sinus
2 patients had h/o PIH . 1 patient had h/o post partum hemorrhage .
RX � anticoagulants � heparin and later warfarin , anticonvulsants, antihypertensives in 2 cases with PIH .
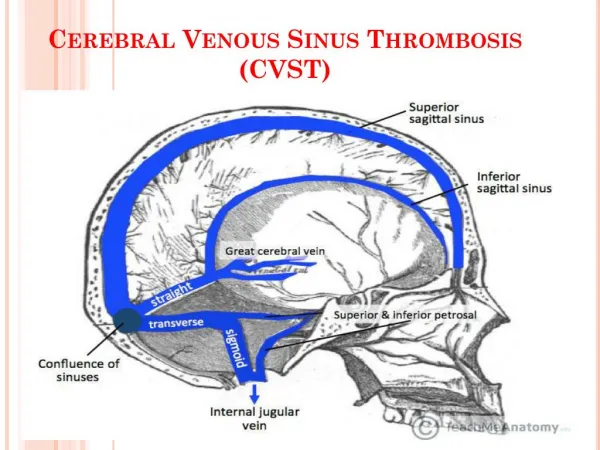
5. CEREBRAL VENOUS THROMBOSIS RIBES- 1825-Known as cortical venous , cerebral sinus , venous sinus, or dural sinus thrombosis
Infrequent condition accounts for 15-20% of stroke in pregnancy
Commonest cause of stroke in young women in India
50% related to pregnancy and puerperium
95.5% - CVT
INCIDENCE : 1 in 1666-10,000 pregnancies
Variable clinical manifestation and mode of onset
Reported mortality- 5-30%
High suspicion required for diagnosis
Early diagnosis and rapid mangement � complete recovery , saves life.
6. PATHOGENESIS Thrombosis of cerebral veins
obstruction of venous return� intracranial hypertension
Localised cytotoxic cerebral edema, venous infarctions
Ischemic neuronal damage , petechiae ?large hematoma
7. CAUSES Endocrinological causes- use of OCP, pregnancy, puerperium,
Hematological �APLA, anemia, coagulation disorders, thrombophilias
Connective tissue disorder- SLE, IBD
Neoplastic � metastasis, glomus tumour
Infective � abscess, meningitis,endocarditis
Miscellaneous- high altitude, cardiac failure
Idiopathic- 25%
8. RISK FACTORS IN PREGNANCY Pregnancy and peurperium- hypercoagulability, venous stasis, endothelial injury.
Advanced maternal age
Multigravida
Use of OCPS-third generation �gestodone,desogestrel (54.3%)
Hypertension
Cesarean delivery
Associated infections
Excess vomiting during pregnancy
Dehydration and increased blood loss
Thrombophilias � (34.1%)
9. Clinical Presentation High index of suspicion is required
1.Headache � 90% of adultS- mimic a subarachnoid haemorrhage rarely
2.Focal presentation
Cerebral lesions and neurological signs � 50%
Unilateral hemispheric symptoms (ie: hemiparesis or aphasia) (cortical lesions on both sides of the superior sagittal sinus)
Seizures � 40%
Delirium, amnesia, mutism- (straight sinus and branches)
Coma , Death- cerebral herniation
3. Cavernous sinus thrombosis- chemosis, proptosis,ophthalmoplagia .
4.Pseudotumour cerebri
headache (can mimick migraine or chronic daily headache), progressive with no other neurological symptoms � exception of diplopia due to involvement of 6th cranial nerve, papilloedemaheadache (can mimick migraine or chronic daily headache), progressive with no other neurological symptoms � exception of diplopia due to involvement of 6th cranial nerve, papilloedema
10. INVESTIGATIONS CT- filling defect in posterior portion of sinus- �Empty Delta Sign�, small ventricle, decreased sulcal pattern, hemorrhagic infarct
MRI- evolves over time, acute phase- absence of normal venous flow void on T1 &T2 weighted images, thrombus appears isotense or hypotense
next 10 days- hyperintense
MRV- filling defects in the principal dural sinus
MRI + MRV � investigation of choice
HELICAL CT VENOGRAPHY
CONVENTIONAL ARTERIOGRAPHY
LUMBAR PUNCTURE
12. Treatment recommended General: supportive, symptomatic
Treatment of underlying cause
Anticonvulsants
Anticoagulation �HEPARIN is first drug of choice
Arrest the thrombotic process and prevent Pulmonary embolus. Tendency of venous infarcts to become hemorrhagic. But anticoagulation is safe , even in the setting of ICH , decreases risk of death and dependency.
LMWH for 5-7 days followed by 3months or more of warfarin therapy in presence of risk factors. In pregnancy � heparin till 12 weeks, then warfarin till 34 weeks and heparin till term.
Endovascular thrombolysis- Urokinase is used
Intracranial hypertension alone � lumabar puncture, oral acetazolamide.
Surgical evacuation of clot , decompressive craniectomy
Mannitol, surgical evacuation of clot or decompressive craniectomyMannitol, surgical evacuation of clot or decompressive craniectomy
13. Prognostic factors- ISCVT Important prognostic factors for death or dependence
Coma (GCS < 9)
Cerebral Haemorrhage
Malignancy
Causes of death- secondary intracranial hemorrhage , transtentorial herniation.
Prognosis unpredictable- permanent visual loss, residual epilepsy, disability, coma, death. Good prognosis if treated early .
Recurrence � h/o CVST does not preclude subsequent pregnancy
14. Pregnancy related VTE and CVST occurs most frequently during the Puerperium - recommend post partum anticoagulation
Mehraein study: Unable to draw conclusion regarding need for prophylactic low dose anticoagulation antepartum
Evidence of a very low risk of recurrent VTE for women with previous extracerebral venous thrombotic events if no thrombophila present or if the previous VTE was associated with a temporary RF
Risk of recurrence increased if thrombophilia present or prior event was idiopathic
Decision for prophylactic anticoagulation may be based on Interval b/w previous CVST and subsequent pregnancy- 80% relapses occur within first 2 yrs.
Pregnancy and Risk of recurrence- recommendations 0/44 patients without thrombophilia or idiopathic clot
3/51 with thrombophilia or idiopathic had a clot0/44 patients without thrombophilia or idiopathic clot
3/51 with thrombophilia or idiopathic had a clot
15. BEWARE!!! INJUDICIOUS USE OF OCPS
CHANGING LIFE STYLE
VAGUE NEUROLOGICAL SYMPTOMS
IN PREGNANCY
ALL CONVULSIONS NEED NOT BE
ECLAMPSIA
16. REFERENCES Cerebral venous thrombosis- Isabelle Crassard; J Neuro-Ophthalmol, Vol 24, No.2 2004
Cerebral venous thrombosis � Brig S Kumarvelu; MJAFI 2008;64
A case of postpartum cerebral venous thrombosis Bette Cole; Journal of Neuroscience Nursing 2006
Stroke in pregnancy and peurperium ; Treadwell & Thanvi; Postgrad Med J 2008
Stroke complicating pregnancy and puerperium; C.-C. Liang & S.-D.Chang ; European Journal of Neurology,2006
Venous thromboembolism , Williams Ostetretics