Lung Cancer Screening
850 likes | 1.28k Views
Lung Cancer Screening. Caryn Gee Morse, MD March 20, 2001. Lung Cancer: the problem . In the United States, the second most common cancer in men and women Leading cause of cancer mortality Accounts for more deaths from than cancer than breast, prostate and colorectal cancer combined.

Lung Cancer Screening
E N D
Presentation Transcript
Lung Cancer Screening Caryn Gee Morse, MD March 20, 2001
Lung Cancer: the problem • In the United States, the second most common cancer in men and women • Leading cause of cancer mortality • Accounts for more deaths from than cancer than breast, prostate and colorectal cancer combined
Common and Lethal • The American Cancer Society estimates 169,500 new cases of lung cancer will be diagnosed in 2001 • Overall 5-year survival remains poor, approximately 15% • ACS anticipates 157,400 deaths from lung cancer in 2001
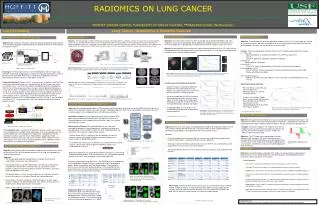
Estimated U.S. Cancer Deaths10 Leading Sites, by Gender 2001
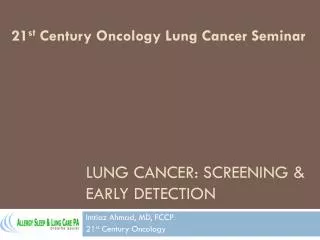
Age-adjusted cancer death rates by siteUS females, 1930-1997
Table 4. Current guidelines for lung cancer screening • Adapted from Mandel, J, Weinberger, S. Screening for lung cancer. UpToDate 2000; 8:1-2. • Mandel, J, Weinberger, S. Screening for lung cancer. UpToDate 2000; 8:1-2.
Presentation overview • History of lung cancer screening • Trials of the 1950-60s • National Cancer Institute Cooperative Early Lung Cancer Project • Mayo Lung Project • Memorial Sloan-Kettering • Johns Hopkins • Czechoslovakian Trial • Lost interest
Presentation Overview Cont. • Renewed interest and new directions • Chest radiographs • Computed tomography • PET • Biomarkers • Fluorescence bronchoscopy • Conclusions and recommendations
Screening Principles Successful cancer screening program: • needs to detect disease in the preclinical stage • when it is amenable to curative treatment • reduce mortality by preventing progression of disease
Lung cancer screening A successful randomized trial of screening for lung cancer: • Enhances detection of lung cancers, particularly asymptomatic, early stage cancers, in the study group when compared to a control group during the screening phase • As the trial progresses, the number of lung cancers in the two groups should equalize as asymptomatic, early stage cancers undetected in the control group grow, spread, and present as symptomatic, advanced stage cancers • If treatment is more effective for asymptomatic, early stage cancers compared with symptomatic, more advance lung cancers, fewer deaths would be expected in the screened group compared to non-screened controls • Model assumes that the bulk of early stage lung tumors progress to lethal disease without detection and early treatment and assumes that early detection reduces mortality
Screening: mortality and survival • No randomized, controlled trial has demonstrated that lung cancer screening leads to a reduction in disease-specific mortality • Mortality vs. survival • Mortality(death rate): # cancer deaths / # patients screened, expressed as deaths per 1000 persons screened per year • Survival: # patients alive following cancer diagnosis / # cancers detected, expressed as a percentage over time
Screening • Mortality can be influenced by selection bias in nonrandomized trials, however, in a RCT, a statistically significant mortality reduction is considered proof of screening effectiveness or at least best evidence for efficacy
Screening: bias • All other measures of outcome can be affected bias, including: • Selection bias: error in patient assignment between groups that permits a confounding variable to arise from study design rather than by chance alone; usually eliminated by randomization • Lead-time bias: mistakenly attributing increased survival of patients to a screening intervention when longer survival is only a reflection of earlier detection in the preclinical phase of disease • Length-sampling bias: Slow growing tumors are detectable longer than fast growing ones and will be preferentially identified by any early diagnosis strategy. Fast growing tumors, with shorter survival, will be left for routine diagnosis. • Over-diagnosis: a portion of detected cancers may have remained indolent and undetected because of patient death from other causes
Early, early trials • In the 1950s and 1960s a number of uncontrolled and nonrandomized controlled studies were performed to evaluate combinations of chest x-ray and sputum cytology screening at various time intervals, ranging up to once every 6 months • Three nonrandomized, uncontrolled trials: • Philadelphia Pulmonary Neoplasm Research Project • Veterans Administration Lung Cancer Screening Study • South London Lung Cancer Study • Two randomized controlled trials: • North London Cancer Study • Kaiser Foundation Health Plan Study
Early, early trials cont. • All of these studies failed to demonstrate a statistically significant mortality benefit from lung cancer screening. • Small cohorts with limited follow-up periods, limiting demonstration of small-moderate improvements or longer-term benefits in mortality
NCI Cooperative Early Lung Cancer Group • In 1971, the National Cancer Institute (NCI) sponsored three large-scale, long-term, randomized controlled trials created to determine “whether a program of lung cancer screening might lead to earlier detection, that is, to finding a larger proportion of lung cancers at a localized, potentially curable stage, and whether with appropriate treatment this would result in a substantial reduction of lung cancer deaths in the screened group.”
NCI Cooperative Early Lung Cancer Group, cont. • Specifically, the trials sought to establish if detection of early lung cancer could be improved by the addition of sputum cytology to routine chest x-ray and if lung cancer mortality could be reduced by this screening and appropriate therapy. • The trials, completed in 1984, were conducted at Mayo Clinic, Johns Hopkins Medical Center and the Memorial-Sloan Kettering Cancer Center and the participating institutions were designated the Cooperative Early Lung Cancer Group.
Mayo Lung Project • From late 1971 to mid-1976, enrolled • 10,933 male volunteers • Age 45 years or older • At least one pack per day cigarette use in the previous year • Referred for participation by their primary care physician during routine physical examination • All participants were offered an initial prevalence screen including chest x-ray and sputum cytology.
Mayo Lung Project • 91 prevalent cancer patients removed from the initial volunteers • 978 patients ruled ineligible because of “serious underlying medical problems” and predicted life expectancy of less than 5 years • 653 volunteers refused participation • Remaining 9211 participants were randomized to two groups, screening and control • Screening group participants received chest x-ray and sputum cytology examination every 4 months for 6 years • Control group participants were advised to seek annual chest x-ray and sputum cytology, “standard Mayo advice” at the time and no reminders were sent • Study group was followed for a total of 9 years, 6 years of screening and 3 years of follow-up observation.
MLP: Late stage cancers, nonresectable cases and number of deaths
Memorial Sloan-Kettering • From 1974 to 1978, enrolled: • 10,040 male volunteers • Age 45 years or older • At least 1 pack per day cigarette use currently or in the preceding year • On initial intake all participants received PA and lateral chest films and pooled sputum cytology
Memorial Sloan-Kettering • Following the initial prevalence screen: • 5072 men randomized to the “chest x-ray only group” • 4985 men randomized to the “dual-screened group” • Both groups received annual chest x-rays. • The dual-screened group additionally received 3-day pooled sputum cytology every 4 months.
M S-K Conclusions • There was no statistically significant difference in early stage lung cancers identified, 5-year survival or mortality between the dual-screen group and the chest x-ray only group • Sputum cytology, even as often as q4 months, does not improve mortality compared to CXR alone
Johns Hopkins • Uncanny-ly similar to Memorial Sloan-Kettering • From 1973 to1977 enrolled: • 10,387 male volunteers • Age 45 years or older • At least one pack per day smoking history in preceding year • Volunteers were randomly allocated to two groups: • Control, or single-screen group, received annual radiographic screening only • Dual-screen group received annual radiography plus annual sputum cytologic examination
Johns Hopkins: Incidence • Lung cancer detected in 396 participants: • 194 in the dual-screen group • 202 in the control group • Over half (51%) of the cancers identified were detected incidentally by chest x-ray or sputum cytology performed outside of the screening protocol • Compared with clinical diagnosis by symptoms, screening by both chest x-ray and sputum cytology identified a greater proportion of the lung cancer cases at an earlier stage • Addition of sputum cytology improved detection of squamous cell lung cancer but did not effect disease-specific mortality
NCI Cooperative Lung Conclusions • Demonstrated improvements in stage distribution, resectability and survival in screened groups • No improvement in disease-specific mortality with screening • Cooperative authors recognize the potential effects of bias, lead-time, length-sampling and over-diagnosis • Role of control contamination, screening non-compliance? • However, they hedge, “It is probable that some patients who had lung cancers detected by screening would have died of their malignancies had they not been detected at earlier stages.”
NCI Cooperative LungRecommendations, 1984 1. If screening for lung cancer is to be carried out, it should be done within the framework of general health care; that is, in the private practitioner's office, HMO, or general medicine clinic. 2. The chest x-ray is the most sensitive method for detection of lung cancer currently available. 3. Sputum cytology is the most effective and specific method of detecting early squamous cell lung carcinoma. Patients with positive sputum cytology in the setting of radiologically occult malignancy have good 5 year survival. 4. Data do not indicate if prolonged survival in prevalent cases of lung cancer represented decreased mortality from disease or reflects one or more screening artifacts.
Czechoslovakian Lung Cancer Study • Began in Czechoslovakia in 1976 • Designed to evaluate semi-annual screening by chest x-ray and sputum cytology • 6364 males, ages 40-64, with a greater than 20 pack year history of tobacco abuse, were screened with PA chest x-ray and 24-hour sputum cytology to identify prevalent cases
Czech study cont. • After the prevalence screen, remaining participants were randomized to a screening group or a control group • 3172 randomized to screening: received PA chest x-ray and sputum cytology every 6 months for 3 years • 3174 randomized to control: received a single screening chest x-ray at the end of the 3 year trial • All participants received annual chest x-ray for an additional 3 years following the screening period
Czechoslovakian Lung Cancer Study Prevalence: • Initial screen identified 19 cancers, 9 squamous cell carcinomas and 7 small cell lung cancers • Overall prevalence was 3/1000 examinations • 5-year survival for prevalent cases was 25%
Czechoslovakian Lung Cancer Study • During the three year screening period, 55 confirmed lung cancers were identified • 36 cases were identified in the screening group. 26(75%) cancers found in asymptomatic participants • 19 cases were identified in the control group. 4 (25%)found incidentally or at autopsy • Following the screening period, annual CXR surveillance revealed an additional 35 cases of lung cancer in the screening group and 38 cases in the control group • Overall mortality after nine years was 3.6/1000 person/years in both the screened and control groups
RCT, summary cont. • Four RCTs collectively screened 37,724 participants • All studies demonstrated improvements in stage distribution, resectability and survival in screened groups • No improvement in disease-specific mortality with screening