Auto-immune diseases
Auto-immune diseases. Leonard H Sigal MD, FACP, FACR P.R.I.- CD& E- Immunology Bristol-Myers Squibb Princeton, NJ Clinical Professor of Medicine and Pediatrics UMDNJ – Robert Wood Johnson Medical School New Brunswick, NJ. “Too little immunity” is a problem.

Auto-immune diseases
E N D
Presentation Transcript
Auto-immune diseases Leonard H Sigal MD, FACP, FACR P.R.I.- CD& E- Immunology Bristol-Myers Squibb Princeton, NJ Clinical Professor of Medicine and Pediatrics UMDNJ – Robert Wood Johnson Medical School New Brunswick, NJ
“Too little immunity” is a problem But, what about “too much” immunity? Recall: Critical to a proper immune response is being able to differentiate “self” from “non-self”- the entity from the attackers
“Too much immunity” • Allergy- one theory: may be due to improved hygiene and lack of ambient bacterial exposures early in life • Auto-immunity- breakdown in tolerance- genetic predisposition plus environmental exposure as trigger
AUTO-IMMUNITY • Breakdown in ability to differentiate “self” from “non-self” • Tolerance is the ability to not immunologically react to self • Self-recognition (non-auto-aggressive behavior) is part of many normal immune and homeostatic mechanisms • 5 to 8% of the US population has an auto- immune disorder, may be more than one
AUTO-IMMUNITY • Tolerance starts in thymus and continues with active suppression in the periphery • Developing “immunocytes” are exposed to self-antigens and if their receptor recognizes self too well the cell is eliminated (“negative selection”); no recognition “positive selection”; mid- ground survive but anergized or controlled peripherally.
AUTO-IMMUNITY • Organ-specific: single or a few • Systemic • Auto-immunity of a single organ often means there is another organ affected • Family history is often positive
Self-recognition- salubrious examples • Idiotype network- regulation of antibody production • Antigen presentation: MHC and cell-surface antigen receptors interact • Ligand-receptor interactions • Antigen-specific suppressor cells & factors
Why auto-immunity? • There are “auto-aggressive” immune clones in your body right now • Under normal circumstances these are kept under control- breakdown in control leads to auto-aggressive behavior • A breakdown in tolerance can lead to auto- immunity • In both SLE and RA, auto-antibodies may be present for up to 9 years prior to disease
What Induces Autoimmunity? CENTRAL (prenatal) and PERIPHERAL (later) MECHANISMS
Aire- a key to tolerance induction in the thymus • Aire- auto-immune regulator: protein expressed in the thymus that induces thymic medullary epithelial cells to express 200 to 1200 non-thymic proteins, seemingly to allow intra-thymic processing and presentation of these proteins to lead to tolerance • Defect of Aire expression associated with APECED: autoimmune polyendocrinopathy candidiasis ectodermal dystrophy
FOXp3 • Mouse strain “scurfy”: develops an X-linked recessive auto-immune disorder with multiple organ-specific inflammation, hypergammaglobulinemia, wasting and a lymphoproliferative disorder- due to uncontrolled activation and proliferation of CD4+ T-cells. • Similar human disease phenotype: • X-linked autoimmunity, allergic dysregulation syndrome (XLAAD) • Immune dysregulation, polyendocrinopathy, endocrinopathy, X-linked syndrome (IPEX).
T-regs: CD4+ CD25+ • GITR, CD62L, CTLA4 or E/7 integrin might be better markers than CD25
non T-reg T regulators • CD4+ TH1 cells (secreting gamma interferon) • CD4+ TH2 cells (secrete IL-4) • CD4+CD25+ TH3 cells (IL-10 and/or TGF) • CD4+ TR1 cells (secrete IL-10) • intraepithelial CD8+ /cells (IL-10) and natural killer T-cells (IL-4).
Adaptive/Acquired Immunity: Activation of Effector T cells Antigen Presenting Cell Foreign antigen Viral antigen Self antigen Processing & Loading MHC class I MHC class II TGF + IL6 TGF CD4+ Helper CD4+ Th17 CD8+ Cytotoxic CD4+ CD25+ Treg Foxp3 IL17 IL22 Effector T cells Possible autoimmune activity Antibodies Cytokines Cytotoxic cell activity TGF IL10 Regulatory functions
CD4 cell populations of note Th1 Th2 Th17 Intracellular Extracellular pathogens Extracellular pathogens like parasites bacteria* IFN IL4 IL17A LTIL5 IL17F TNFIL6 IL6 IL2 IL9 IL10 IL13 * Bacterial species implicated include : Klebsiella pneumoniae, Bordetella pertusis, Citrobacter rodentium, and Borrelia burgdorferi
Macrophage T Cells Orchestrate the Adaptive and Innate Responses Proliferate and differentiate to effectors CD4+ T-helper cell Osteoclast RANK-L T cell T cell IL-2 IL-4, IL-10 T cell T cell B-cell IFN-g, TNF-a IFN-g IL-4 IL-5 TNF-a TGF-b IL-3, IL-7, GM-CSF Stem cell B-cell proliferation B-cell differentiation cytokine production APC activity antibody production TNF-a, IL-1, IL-6, IL-12
DC DC Chr. inflam Tcell Tcell Ag Ag Chr. oxid. Bcell Bcell C3 Suppressive networks Suppressive networks C3a 1. Genes 2. Abnormal Immune Response 4. Inflammation 5.Damage C1q,C2,C4 HLA-D2,3,8 MBL FcR 2A,3A,2B IL-10 MCP-1 PTPN22 Environment Rash Nephritis Arthritis Leukopenia CNS dz Carditis Clotting Etc Renal Failure Atherosclerosis Pulm fibrosis Stroke Damage from Rx Etc 3. Autoantibodies Immune Complexes UV light Gender EBV Other Infe Others Courtesy Bevra Hahn, MD
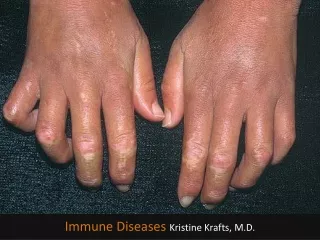
Auto-antibodies- receptor targets:Receptor Stimulate Block • TSH R. Graves Hashimoto’s • Insulin R. Hypo- Hyperglycemia • ACTH R. Addison’s • Intrinsic Factor Pernicious anemia • ACh R. Myasthenia gravis
Auto-antibodies- other targets: • Basement membrane Goodpasture’s syndrome • Uveal tract Sympathetic ophthalmia • Cardiac tissue Dressler’s syndrome • Exocrine glands Sjogren’s syndrome • Epidermal Bullous pemphigus hemidesmosomes • Blood cells Hemolytic anemia, AITP
TREATMENT OF AUTO-IMMUNITY • If hormonal deficiency- REPLACE • If organ inflammation- SUPPRESS Pulse corticosteroids Oral corticosteroids Cytotoxic agents Immunomodulatory agents Plasmapheresis
TREATMENT OF AUTO-IMMUNITY • Neutralize inflammatory cytokines: Solubilized receptor TNF Monoclonal antibody TNF, BLyS Antibody to receptor IL-6 Receptor antagonist IL-1 • Suppress antigen-specific response Co-stimulation blockade CTLA4Ig • Counterbalancing cytokines
MP/DC Clinical Trials Treg IFNa Anti-IFNa Edratide DR B7 LJP394 Peptide CD28 TCR X Y Anti-CD20 BCR CD20 Anti-CD22 CTLA4-Ig CD22 T Cell B Cell CD28 B7 IMPDH IMPDH Inosinic acid purines Inosinic acidpurines BCMA APRIL BLyS Mycophenolate Mycophenolate Anti-BLyS TACI-Ig Courtesy Bevra Hahn, MD
Molecular biology has given us a new therapeutic world • Replace deficiencies- IVIG, ADA • Repair genetic defects- ADA • Stem cell transplants • Cytokines, receptors, antibodies- antagonist and agonist • Support patients until defect identified and toxicity of therapy can be overcome
Abbreviations in common use • SUFFIXDESCRIPTION • -mab Monoclonal antibodies • -umab Human mab • -ximab Chimeric mab (mixture of mouse and human structures) • -zumab Humanized mab (very short murine sequences remain, solely in the antigen-binding regions) • -cept Receptor-antibody fusion protein, often Fc component of an IgG • -kinra Interleukin receptor antagonist (-kin is suffix for interleukin; -ra for receptor antagonist) -nakinra IL1 receptor antagonist • -tinib Inhibitor of a tyrosine kinase
SYSTEMIC INFLAMMATORY SYNDROMES • Systemic lupus erythematosus (SLE) • Rheumatoid arthritis (RA) • Juvenile rheumatoid arthritis (JRA)- aka Juvenile idiopathic arthritis (JIA) • Juvenile dermatomyositis • Kawasaki disease • Seronegative spondylarthropathies (SNSA)
SYSTEMIC LUPUS ERYTHEMATOSUS • Multi-system inflammatory disease • Episodic features in kidneys, brain, skin, joints, serosa • Broad range of severity • Steady improvement in outcomes with the evolution of better treatment • Poor outcome: CNS or renal disease; lower socio-economic status; “externalized locus of control”
Constitutional Skin: malar rash, discoid lesions, photosensitivity Oral/nasal muco- cutaneous lesions Joints and Muscle Nephritis Brain: seizures, psychosis Pleurisy/pericarditis Cytopenias Positive ANA Immunoserologies: dsDNA, Sm, anti- cardiolipin SYSTEMIC LUPUS ERYTHEMATOSUS-Criteria Need “4 of the 11” criteria
SYSTEMIC LUPUS ERYTHEMATOSUS • Most common cause of death used to be: active disease • Now, it is consequences of STEROIDS: early: infection late: accelerated atherosclerosis • Consequences of cyclophosphamide: malignancy • Consequences of dialysis, hypertension, etc. end-organ damage
IL-10 Ts TGF TGF IFN Crow MK, A&R, 2003
Treg (Foxp3 CD4+ T) are Depleted in Patients with Active SLE Miyara et al, J Immunology, 2005
TGF in Normals T CD8 B TGF IL-2 AB NK NK Treg CD4
Patients with SLE Make Abnormally Low Levels of TGF TGF pg/ml * * Ohtsuka et al, JI 1998 Human cells stimulated with anti-CD2
SYSTEMIC LUPUS ERYTHEMATOSUS • Therapy tailored to the organ system(s) affected, severity/type of damage • NSAIDs • Hydroxychloroquine • Corticosteroids • Cyclophosphamide • Azathioprine • Biologics in trials- BLyS, CTLA4Ig
Rheumatoid arthritis • 1% of population; seems to be decreasing in incidence • Synovitis, primarily of small joints of hands and feet • Symmetric- could this be neural input? • Rheumatoid factor • Anti-CCP (cyclic citrullinated peptide) prior to disease
Rheumatoid arthritis- focus? • T cell • Macrophage • Synoviocyte (fibroblastoid) • B cell • Genetics • Anti-CCP2
Rheumatoid arthritis- therapies • NSAIDs, COX2s • Corticosteroids • Methotrexate, leflunomide • Cyclosporine (T cell target) • Anti-CD3; total nodal irradiation • Anti-TNFs • Co-stimulation modulation • B cell assassination; B cell activation blockade
JUVENILE IDIOPATHIC ARTHRITIS (JIA)-ILAR 1995 • Seven categories: • Systemic • Oligoarthritis • Polyarthritis (RF-) • Polyarthritis (RF+) • Psoriatic arthritis • Enthesitis-related arthritis- related to SNSAs • Other arthritis
JUVENILE RHEUMATOID ARTHRITIS (JRA)/ IDIOPATHIC ARTHRITIS (JIA) • Unknown etiology • Unknown immune focus in joints, eyes, etc. • Age < 16 years at onset • Genetic pre-disposition • Multiple cytokines involved, e.g. TNF, IL-1, IL-6
Macrophage Activation Syndrome- complication of systemic JRA • Acute onset- high fever, lymphadenopathy, acute hepatitis, profound cytopenias, DIC • Can be post-viral, NSAIDs, Methotrexate • Can mimic JRA flare • Hematophagocytosis by well-differentiated macrophages in bone marrow • Rx?: steroids, IVIG, cyclosporin
Macrophage activation syndrome Myelocyte within activated macrophage, and multiple adherent red blood cell and myeloid precursors.
Macrophage activation syndrome Neutrophilic bands and metamyelocyte within an activated macrophage.
JUVENILE IDIOPATHIC ARTHRITIS- New management • Methotrexate • Etanercept • Infliximab • Adalimumab • Leflunomide • Abatacept (CTLA4-Ig) • Anakinra not very effective • Anti-IL-6 effective; not yet approved
DERMATOMYOSITIS • Multi-system inflammatory disease • Adults and children • Acute and chronic inflammation of striated muscle and skin
SERONEGATIVE SPONDYLOARTHROPATHIES • Ankylosing spondylitis • Psoriatic arthritis • Psoriatic spondyloarthropathy • Inflammatory joint disease associated with inflammatory bowel disease • Reactive arthritis (no longer called Reiter syndrome)
SERONEGATIVE SPONDYLOARTHROPATHIES • No serum rheumatoid factor • Inflammation of spine and sacroiliac joints • Primary focus of inflammation is the enthesis • HLA-B27: independent linkage with aortic disease (and anterior uveitis)
SNSA- therapy • NSAIDs, COX2 • Sulfasalazine • TNF blockade
SYSTEMIC INFLAMMATORY SYNDROMES-Vasculitis • Classified by size of vessel affected Large: Takayasu Medium: PAN; Churg-Strauss Medium: Wegener; Goodpasture Small: Henoch-Schonlein Purpura • Pathogenesis is unclear: immune complex; auto-antibody; cellular reactivity
COMBINATIONS OF FEATURES GREATLY ENHANCE PROBABILITY OF VASCULITIS Fever Glomerulonephritis Palpable purpura Peripheral neuropathy Established auto-immune disease Ischemia, e.g. gut, heart, brain especially in young patients