Download

1 / 23
240 likes | 440 Views
Third Line of Defense Part II—B cells and antibodies. B lymphocytes (B cells). B cells look exactly like T cells and NK cells. B cells mature in the bone marrow (not the thymus gland, like T cells).

E N D
B lymphocytes (B cells) B cells look exactly like T cells and NK cells. B cells mature in the bone marrow (not the thymus gland, like T cells). Like other APCs, B cells have Class II MHC receptors on their surface. However, they also have another receptor molecule on their surface—antibodies. Upon phagocytosing (word??) an antigen, the antigen is presented, and recognized by a Th cell. See page 362, Table 13.6. This interaction triggers the B cell to differentiate (take on new function) as a plasma cell.
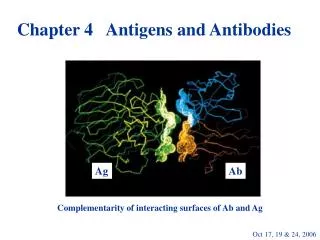
Plasma cells (still lymphocytes) now mass produce antibodies. What are antibodies??? Antibodies are proteins which bind specifically to antigens. Antibodies have a unique characteristic shape:
The antibody protein is made of four polypeptide chains that form the letter Y. The bottom of the Y is the fc portion (constant fragment). The “arms” of the Y are the fab fragments (antigen binding fragment) In B cells, antibodies are bound to the membrane at the Fc site. Plasma cells secrete antibodies into the blood. Fab sites Fc site
The Fab sites are “hypervariable.” A given antibody matches a unique antigen. The host DNA is able to create these unique proteins by recombining within a plasma cell (“jumping genes.”) Antibodies are commonly called “immunoglobulins” (Ig) and are of five types. Each type can be distinguished biochemically: they are of distinctive sizes and (in some cases) shapes.
Remember: MADGE IgG: (gamma globulin): The most common type. Produced by B cells, B memory cells, and plasma cells. Produced in high numbers during a secondary immune response (explained below). IgG is the only antibody type that crosses the placenta.
IgE:Produced by mast cells (tissue) and basophils (leukocytes). Binds to allergens during an allergic response. When IgE binds, the mast cells/basophils degranulate, release cytokines (chemicals) that trigger the symptoms of an allergic response. IgE protects from parasitic infections, but under most circumstances, they cause more health problems than they solve.
IgD:Produced by B cells in very low concentrations. Function: ??????????
IgM: This is the first antibody to be produced in response to an infection. Exists as a pentamer: five immunoglobulin molecules bound to a central piece. Produces the same protection as IgG, but slower and less potent. However, there are 10 Fab sites (compared to two as IgG has).
IgA:Two subunits (dimer). Produced at mucous membranes in secretions (mucus, saliva, tears, breast milk, vaginal fluids, semen). Provides a specific feature to the First Line of Defense.
So, now that you’ve seen the five antibody types, how do antibodies fight pathogens? 1) exotoxins, bacterial proteins (flagella, capsules, fimbrae): Antibodies bind these directly and make them non-toxic. Later, the antibody/antigen complexes can be phagocytosed or eliminated by the liver. The bad news: antibody/antigen complexes that are not eliminated can obstruct capillaries or collect in joints (serum sickness)
Complement fixation Complement (review: a cascade of proteins in the Second Line of Defense) Complement can be activated by antibodies that have bound to antigen (IgM and IgG only). This increases the chances that they will lyse the cell. Usually bacteria are killed this way.
Opsonization When antibodies bind to non-self antigens, they change surface charges on the antigens, which makes them more likely to be attacked by phagocytes. This process of making the antigen more “attractive” to phagocytosis is called opsonization.
Antibody concentration is called titer First exposure to antigen: Sensitizing dose. • Latent phase: no antibody titer at first. This is when antigen is recognized by antibodies on the surface of B cells, the B cells differentiate into plasma cells by interaction with Th cells.
Primary response: First antibody to rise in titer is IgM. Titer rises, then falls (2-4 weeks). This rise in IgM titer is followed by a similar rise in IgG titer (delayed by a week or two). The IgG titer falls somewhat, but remains elevated long after the primary response ends.Clinically, the patient is having the expected reaction to the pathogen. Depending on the portal of entry, the rise in IgG may also be a rise in IgA or even IgE (if it’s an allergen)
Secondary response: The second exposure to antigen (sometimes called the “shocking dose”), causes an immediate and rapid increase in IgG titer. There is also a slight increase in IgM. Antibody responses (neutralization, opsonization, or complement fixation) are rapid and thorough.Clinically, with an effective antibody response, the patient is unaware that anything has happened.
Types of immunity: • Natural: occurs without man-made intervention • Artificial: medical science has induced the immunity. • Active: the patient mounts his/her own immune response • Passive: the patient receives immune cells or antibodies (s)he has not produced.
Vaccination: artificial active immunity • Edward Jenner—1796. Determined that injecting people with serum from cowpox (a minor skin irritation) made them immune to smallpox (a devastating fatal disease). • Vaccination: creating an antibody response by sensitizing the patient to antigens of a pathogen without exposing them to the pathogen itself.
Usual vaccine types: • Pieces of antigens (toxoids) • Dead pathogens (Salk polio vaccine, influenze) • Live attenuated (non-virulent) pathogens (Sabin polio vaccine)Live viruses are often maintained in raw eggs.
Connection between vaccines and autism: MYTHBUSTED!!!!!
Additional uses for antibodies in medicine Because antibodies are specific to given pathogens, they can be used as a diagnostic tool. • Antibodies can be complexed to latex particles in suspension. This allows identification of antigens in many clinical specimens (e.g. Staph aureus, C.diff, meningitis organisms, tuberculosis). This is a way to eliminate the need for culture if there is no time.
Blood banking: anti-A, anti-B, anti-Rh, crossmatching. • Antibody testing can be against bacterial capsules, flagellae, or fimbriae (Salmonella) • Can create antibodies against other antibodies! We create antibodies to human IgG in rabbits (HIV test) • Antibodies can be “tagged” with radioactive isotopes, fluorescent compounds, or colored enzymatic compounds (RIA, ELISA) to allow rapid and extremely sensitive detection of antigens.