Download
1 / 89
1.08k likes | 1.97k Views
Approach to Low Blood Counts: Thrombocytopenia. by Melanie Bodnar MD FRCPC (April 2010) Teaching materials originally developed by Anthony Woods, MD, FRCPC. Overview of Lectures:. Wednesday: introduction to the CBC approach to anemia approach to neutropenia Thursday:

E N D
Approach to Low Blood Counts: Thrombocytopenia by Melanie Bodnar MD FRCPC (April 2010) Teaching materials originally developed by Anthony Woods, MD, FRCPC
Overview of Lectures: Wednesday: introduction to the CBC approach to anemia approach to neutropenia Thursday: approach to thrombocytopenia brief overview of bleeding disorders Review of venous thromboembolic disease Friday: Case presentations and problem solving
Objectives • Classify bleeding disorders: primary vs secondary hemostasis • Bleeding risk assessment • Use pathologic categories to develop a differential diagnosis for low platelets • Investigations for low platelets • Recognize low platelet emergencies
Hemostasis • Hemostasis = stop flow of blood • To orient us to the role of platelets • To understand how bleeding with low platelets may present in contrast to problems within the coagulation pathways • To discuss screening “tests” for bleeding risk
Principles of Hemostasis 1. Primary Hemostasis: Vascular response & platelet plug formation 2. Secondary Hemostasis: Fibrin clot formation 3. Resolution:Fibrinolysis
HEMOSTASIS 2. Secondary hemostasis - fibrin clot 1. Primary hemostasis-platelet plug Subendothelium
HEMOSTASIS 3. Resolution-fibrinolysis and wound healing Subendothelium
Assess Patient for Bleeding Risk • Patients undergoing a surgical or interventional procedure should be screened for a bleeding disorder • Screening: • bleeding history • simple lab tests: CBCd, blood film, INR, PTT
BLEEDING HISTORYThe most important “test” • HPI: • Is there a history of bleeding with surgery, dental work or previous pregnancies? IF YES: • When did the bleeding start? • Quantify the bleeding? • Other sites of bleeding? • Is there SUPERFICIAL (petechiae, ecchymoses, mucosal) or DEEP tissue (joint, muscle) bleeding? • Spontaneous bleeding or bleeding with trauma? • If after trauma is it immediate or delayed?
BLEEDING HISTORY • PHMx: • In women, is there a history of excessive menstrual bleeding leading to iron deficiency? • Any other medical illnesses: liver disease, renal disease, connective tissue disease • MEDS: • ASA, antiplatelet medications, anticoagulants • OTC (NSAIDS) /herbal medications • Family hx: • Who and what type of bleeding problems?
Lab tests to screen for bleeding risk • Complete blood count and peripheral smear • Coagulation: • PT / INR • PTT • Other tests for systemic disease as guided by history and physical plt count? any red flags that a bone marrow problem may be present? Abnormal looking plts? Increased INR or PTT or both raise possibility of factor deficiency (ie hemophilia), but there is a broad ddx
No further testing required IF: • Negative history • Normal CBCd, blood film, INR, PTT • Further testing required consult with hematologist IF: • Suspicion of bleeding disorder raised on history, but normal lab tests • Abnormal lab tests • Abnormal history AND labs N.B. The above lab tests may be NORMAL in many different serious bleeding disorders the history is important!
thrombocytopenia like anemia, thrombocytopenia is defined according to laboratory values: normal @ the UofA is 140 – 450 x 109 / L a platelet count less < 140 is thrombocytopenic also like anemia, thrombocytopenia is not a diagnosis, but a lab value that must be explained 17
Petechiae Oral blood blisters
Thrombocytopenia: • Low platelets are often found serendipitously on blood work • Symptoms tend not to be evident until the platelet count drops below 30 or even 20 • Nonetheless, it is still important to determine the cause of the low platelets and to characterize the platelet count drop by following repeated CBC
Thrombocytopenia like anemia, there is a very long list of conditions that can lead to a low platelet count Classification by pathologic category is the most useful Alwayswant to exclude the most serious, life-threatening causes of low platelets: some of these causes are TRUE EMERGENCIES
Low platelets: pathologic categories ↓ production things that affect marrow 2. ↑ destruction either immune or 20 to blood vessel abnormalities or microvascular thrombosis sequestration spleen or dilutional
ITP (immune thrombocytopenia) common • DIC • TTP • HIT Life threatening!!
ITP - pathophysiology destruction in reticuloendothelial system (spleen, liver) 26
Immune thrombocytopenia In children: more common in those under 6 yrs often follows a history of viral URI spontaneous recovery & infrequent recurrence platelet counts can be very low (less 10) Rx: -observation if no bleeding -intravenous Immunoglobulin (IVIG) -steroids 2nd line (try to avoid) -splenectomy for life-threatening bleeding only—want to avoid this in kids because of increased risk of infection and most will remit with time 27
Immune thrombocytopenia In adults tends to be a CHRONIC disease: more common in young women Does increase bleeding risk, but major hemorrhage surprisingly rare platelet counts can be variable (mild to very severe) waxing and waning course long-term remissions rare goal of therapy is prevention of bleeding Rx: IVIG for acute bleeding steroids are first line therapy splenectomy is 2nd line therapy other steroid sparing treatments 28
Immune thrombocytopenia Immune thrombocytopenia purpura (ITP) is a diagnosis of exclusion can only be diagnosed after reasonable investigations are negative in an otherwise healthy person in patients older than 60, a bone marrow examination may be included chances of a malignancy or myelodysplastic syndrome increase in this age group 29
Several investigations warranted in the work-up for ITP (recently published guidelines) specialist • BUT! A key component in the work up of low platelets is to RULE OUT life-threatening emergencies • every physician should know about these and the tests required to exclude them
The three-letter low platelet EMERGENCIES DIC= disseminated intravascular coagulation TTP = thrombotic thrombocytopenic purpura HIT = heparin induced thrombocytopenia PTP Post-transfusion purpura– rare cause of low platelets (usually <10) associated with recent red cell transfusion (previous 7-10 days) in genetically susceptible individual
Disseminated Intravascular Coagulation (DIC) not a disease in itself, but a syndrome secondary to some other underlying grave systemic illness
DIC - pathophysiology platelet consumption 20 to coagulation derangement for more detail, see Appendix
DIC – Clinical Picture low platelet count on CBC occasional red cell fragments on smear bleeding oozing at IV sites, venipuncture GI, gum and nosebleeds thrombosis digital infarcts, stroke/neurologic events end-organ damage other lab abnormalities anemia – bleeding, fragmentation hemolysis prolonged PT, PTT, depleted clotting factors low fibrinogen BLEEDING AND CLOTTING YIKES!
DIC - Therapy must treat underlying disease first if patient is bleeding, can replace factors with plasma (replaces clotting factors) and cryoprecipitate (replaces fibrinogen) if thrombosis dominates, low dose heparin can be used others: protein C, antithrombin high mortality
Microangiopathic Hemolytic Anemia = MAHA thrombotic thrombocytopenic purpura TTP hemolytic uremic syndrome HUS
TTP and HUS are both manifestations of microangiopathic hemolytic anemia characterized by: 10 platelet activation & consumption Activation of coagulation cascade with fibrin deposition in vessels leading to red cell fragmentation hemolytic anemia – Hb drops low platelets with hemolytic anemia and red cell fragmentation on blood film is all that is required to make the diagnosis
Patients with TTP may also present with: • Fever (general malaisem flu-like illness) • Renal failure (increasing creatinine) • Neurologic symptoms (transient or more sustained, vague or localized) BUT the absence of these does NOT make TTP less likely
TTP vs HUS there are some clinical differences, but overall, more similarities between them 1 • 1. Common is not the right word….more likely to be seen in TTP than HUS
TTP / HUS - pathophysiology ultimately, a depletion of a vonWillebrands factor cleaving protease (ADAMTS13) is responsible for the syndrome
blood vessel wall no abnormal clotting protease VLVWF absent protease abnormal clot VLVWF normal VWF protease deficient blood vessel wall
fibrin strand red blood cells passing through these clots in small vessels suffer shearing forces microangiopathic hemolysis haptoglobin Hb bilirubin LDH reticulocyte counts RBC activated platelet vessel cross-section
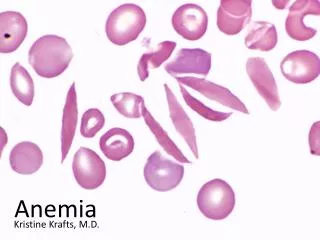
Fragments or schistocytes seen in TTP (MAHA); arrow is pointing to a polychromatophilic cell = reticulocyte
HUS HUS is ‘hamburger disease’ shiga-like toxin from E. coli 0157:H7 (often bloody) diarrhea preceding HUS therapy: Supportive care Detoxification treatments have been explored ? plasma exchange
TTP TTP: associations idiopathic familial – 20 enzyme deficiency (rare) drugs (cyclosporine, ticlopidine, quinine) pregnancy-related transplantation infections (HIV) collagen vascular diseases (SLE, scleroderma) malignant hypertension
TTP is a medical EMERGENCY! Patient needs to be urgently transferred to the care of a hematologist in a centre that can do plasma exchange Without this therapy, mortality approaches 80-90% Support while arranging transfer: avoid platelet transfusions Give 2 units of FFP Other treatments: Steroids treat any underlying cause stop any offending drug
Heparin-induced Thrombocytopenia (HIT) a strong prothrombotic disease state causes a syndrome of low platelets and potent thrombosis arterial or venous clotting May develop life-threatening thrombosis MUST ALWAYS be considered when a patient is on heparin or has recently stopped heparin regular platelet counts while patient is on heparin therapy
platelet • activated platelet • microparticles and • secreted pro-thrombotic • substances • low platelets • tendency to clot ! IgG against complex autoactivates platelet adsorbed complex of PF4 and heparin