
Goals
E N D
Presentation Transcript
Webcast Session IIAn Introduction to Evaluation and Management (EM) CodingAccurate Coding for Evaluation and Management (EM) ServicesA webcast designed for headache and migraine specialistsPresentersStuart B. Black, MDAmerican Headache Society (AHS)Sheila J. Madhani, MA, MPH, CCS-PMARC Associates October 16, 2007
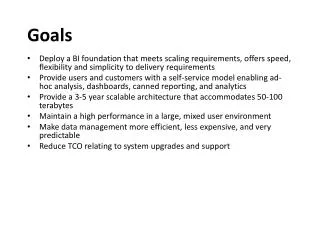
Goals • Introduction to CPT EM codes • How to properly select the appropriate level of Medical Decision Making (MDM) for a specific EM encounter • Application of CPT coding guidelines and practices to clinical scenarios relevant to headache specialists
What Will We Discuss? • Importance of accurate coding • Key components of EM codes • How to properly select the appropriate level of Medical Decision Making (MDM) for a specific EM encounter • General principles of medical record documentation • Clinical examples • Coding resources
Importance of Accurate Coding • Full and fair description of services provided • Avoid over-coding (fraud and abuse) and under-coding (not reporting all the services you have provided) • Improve quality of patient care
Importance of Accurate Coding • Physicians use EM codes to report professional services • Documentation in the medical record must support the EM code and ICD-9 code(s) submitted • Submitting a code that is not supported by documentation may be considered fraud
Key Components of EM Codes • Three key components must be considered and supported by documentation in the medical record before selecting a code • History • Examination • Medical decision making (MDM)
Key Components History • Summary
Key ComponentsPhysical Examination • Summary – 1997 Guidelines, Single System Specialty Exam, Neurological
How to properly select the appropriate level of Medical Decision Making (MDM) for a specific EM encounter
Medical Decision Making (MDM) • What is medical decision making (MDM)? • MDM refers to the complexity of establishing a diagnosis and/or selecting a management option • Of the three key components of EM, MDM is the most challenging to meet and document
Medical Decision Making (MDM) • MDM Factors • Factor #1: Number of diagnoses or management options • Number of possible diagnoses • Number of options that must be considered • Levels • Minimal • Limited • Multiple • Extensive
Medical Decision Making (MDM) • MDM Factors • Factor #2: Amount and/or complexity of data to be reviewed • Amount and/or complexity of medical records, diagnostic tests and/or other information that must be obtained, reviewed and analyzed • Levels • Minimal or none • Limited • Moderate • Extensive
Medical Decision Making (MDM) • MDM Factors • Factor #3: Risk of complications and/or morbidity or mortality • The risk of significant complications, morbidity and/or mortality associated with the patient’s presenting problem • The risk of comorbidities associated with the patient’s presenting problem • The risk of the diagnostic procedure(s) and/or the possible management options • Levels • Minimal • Low • Moderate • High
Medical Decision Making (MDM) • What are the different levels of MDM? • Straightforward • Low complexity • Moderate complexity • High complexity
Medical Decision Making (MDM) • How do I determine the level of MDM for a specific EM encounter? • The level of MDM is based on the level of complexity of the 3 factors of MDM • Number of diagnoses or management options • Amount and/or complexity of data to be reviewed • Risk of complications and/or morbidity or mortality
Medical Decision Making (MDM) • How do I determine the level of MDM for a specific EM encounter? • The level of MDM is based on the level of complexity of the 3 factors of MDM
Medical Decision Making (MDM) • The next few slides provide the following guidance • Issues to consider when determining the level of complexity of the 3 factors of MDM • Recommendations for documenting MDM • Based on 1997 EM Guidelines, Centers for Medicare and Medicaid Services (CMS)
Medical Decision Making (MDM) • Factor #1: Number of diagnoses or management options • Issues to consider • MDM is easier for a diagnosed problem than for an identified but undiagnosed problem • Problems which are improving are less complex than problems that are worsening or failing to change as expected • The need to ask advice from an outside source is an indication of complexity of diagnosis
Medical Decision Making (MDM) • Factor #1: Number of diagnoses or management options • Documentation recommendations • An assessment, clinical impression or diagnosis should be documented • Initiation of treatment or changes in treatment should be documented • Any referrals or consultations, advice sought should be documented
Medical Decision Making (MDM) • Factor #2: Amount and/or complexity of data to be reviewed • Issues to consider • The type of diagnostic testing ordered or reviewed • Decision to review old medical records and/or obtain history from a source other than the patient increases complexity • Discussion of contradictory or unexpected results with the physician who performed or interpreted test increases complexity
Medical Decision Making (MDM) • Factor #2: Amount and/or complexity of data to be reviewed • Documentation recommendations • Any of the following tasks should be documented • Any diagnostic services ordered, planned or scheduled • The review of lab, radiology and/or other diagnostic tests • Decision to obtain old records or obtain additional history from other sources that the patient • Relevant findings from the review of old records and/or additional history • Discussion of diagnostic tests with the physician who performed them • The direct visualization and independent interpretation of an image, tracing or specimen
Medical Decision Making (MDM) • Factor #3: Risk of significant complications, morbidity, and/or mortality • Issues to consider • Risk associated with the presenting problem • Risks associated with the diagnostic procedure(s) • Risks associated with the possible management problems
Medical Decision Making (MDM) • Factor #3: Risk of significant complications, morbidity, and/or mortality • Documentation recommendations • Any of the following risks should be documented • Comorbidities/underlying diseases • Surgical or invasive diagnostic procedures ordered, planned or scheduled at the time of the EM • Any invasive or surgical diagnostic procedure performed at the time of the EM encounter • The referral for or decision to perform a surgical or invasive diagnostic procedure on an urgent basis
Medical Decision Making (MDM) • Risk Table • CMS has developed a risk table to help determine the level of medical decision making for a specific EM encounter (minimal, low, moderate, high) • Table includes common clinical scenarios • Table provides an assessment of risk in 3 categories • Presenting problem(s) • Diagnostic procedure(s) ordered • Management options selected • Highest level of risk in any 1 category determines the overall risk
Centers for Medicare and Medicaid Services (CMS), Documentation Guidelines for EM, 1997.
Key Components Medical Decision Making (MDM) • Table of Risk • For headache specialists the most important risk categories are: • Number of treatment options • The levels of risk complications and/or morbidity or mortality
Medical Decision Making (MDM) • Table of Risk Comparison – elements relevant to headache specialists extracted from Table of Risk
Medical Decision Making (MDM) • MDM scoring system • Methodology to determine level of MDM developed by private organizations • There are several systems currently in use • Based on a point system that takes qualitative information collected by the provider and translates it into quantitative data • More points; higher level of service • Example that follows was developed by the American Health Information Management Association (AHIMA) • In general scoring systems are not part of any CMS guidelines or recommendations
Medical Decision Making (MDM) • MDM scoring system example • Factor 1: Number of Diagnoses or Treatment Options (more than 1 may apply)
Medical Decision Making (MDM) • MDM scoring system example • Factor 2: Amount/Complexity of Data Reviewed (more than 1 may apply)
Medical Decision Making (MDM) • MDM scoring system example • Factor 3: Risk of significant complications • Minimal • Low • Moderate • High
Medical Decision Making (MDM) • MDM scoring system example
Medical Decision Making (MDM) • Summary
Choosing an appropriate level of EM service • Based on Key Components • The three key components must be considered and supported by documentation in the medical record before selecting a code • History • Examination • Medical decision making (MDM)
Choosing an appropriate level of EM service • New patient, office/outpatient and office consultations • You must meet or exceed ALL of the requirements to qualify for a particular level of an EM service • Established patient, office/outpatient • You must meet or exceed 2 out of the 3 requirements to qualify for a particular level of an EM service
Summary • New Patient – Office/OP (3 out of 3)
Summary • Office or other Outpatient Consultation (3 out of 3)
Summary • Established Patient – Office/OP (2 out of 3)
Time • Time determines the level of E/M service when counseling and/or coordination of care dominate (> 50%) the encounter • Counseling and coordination is separate from the history, physical exam and medical decision making • More common scenario for headache specialists • The extent of counseling and/or coordination of care must be documented in the medical record independent of the three key components
Documentation • General Principles of Medical Record Documentation¹ • Medical record should be complete and legible • The documentation of each patient encounter should include: • Reasons for the encounter and relevant history, physical examination findings and prior diagnostic test results; • Assessment, clinical impression or diagnosis; • Plan for care; and • Date and legible identity of the provider • If not documented, the rationale for ordering diagnostic and other ancillary services should be easily inferred ¹ 1997 EM Guidelines, Centers for Medicare and Medicaid Services (CMS)
Documentation • General Principles of Medical Record Documentation¹ • Past and present diagnoses should be accessible • Appropriate health risk factors should be identified • Patients progress and response to changes in treatment should be included • CPT and ICD-9 codes submitted should be supported by documentation in the medical record ¹ 1997 EM Guidelines, 1997 EM Guidelines, Centers for Medicare and Medicaid Services (CMS)
Documentation • Elements of a consultation • There are three documented elements that comprise a consultation • A written request, asking a question, for specific advice or specific management direction in the care of a patient • Documentation of the patient evaluation • A specific written response i.e. the answer to the question, as simple as “Yes, the patient didn’t have a PE and you may proceed with the surgery” • The unspoken fourth component- all of the above must materially contribute to the evaluation and/or management of the patient or the consult is not medically necessary
Case #1 – History (HPI, ROS, PFSH) 70 yr old man with hx of DM. 6 months ago developed herpes zoster; right V1 distribution. After Rx of acute zoster developed constant, deep burning pain in V1 (R) with tic like pain and pain to light touch. Also developed severe (R) hemicranial headaches Under care of PCP; pain refractive to Rx. Referred to H/A Specialist for consult.
Case #1 Pre-service • Reviewed all the patient’s referral records. Reviewed the medical history form completed by the patient, vital signs, additional information obtained by PA. Personal communication with referring physician Intra-service • Comprehensive H&P performed • Reviewed relevant data, risks, and explained clinical features of Post Herpetic Neuralgia • Discussed diagnostic and therapeutic options • Discussed recommended treatment plan Medical Decision Making • Number of Diagnoses or Treatment Options > 4 • Amount / Complexity of Data Reviewed > 4 • Using the Table of Risk: • “Acute or chronic illnesses or injuries that pose a threat to life or bodily function, e.g.. multiple trauma, acute MI, pulmonary embolus, progressive severe rheumatoid arthritis, psychiatric illness with potential threat to self or others, peritonitis, acute renal failure” • “Drug therapy requiring intensive monitoring for toxicity” .
Case #1 Post-service • Complete medical record documentation and send written report to referring physician • Post 1st visit communicate with referring doctor and treat any treatment failures or AE’s if need • Receive and respond to any interval testing results or correspondence • Revise treatment plan if necessary and communicate with patient as necessary The level of care would meet CPT criteria for an Office Consultation 99245. It includes a comprehensive H & P and MDM of high complexity. There has been no transfer of care.
Case #2 – History (HPI, ROS, PFSH) 27 year old woman, established pt, seen in follow up B/O MOH. Post hospital visit following detoxification week ago. Detailed review of post hospital instructions; discussed all medications; discussed Dx and risks of MOH; discussed situation with family and importance of family support. Scheduled for support group.
Case #2 Pre-service Reviewed medical record and hospitalization in detail before encounter with patient and her family. Intra-service Counseling and Coordination of care comprised more than 50% of the encounter; in fact it comprised 100% of the encounter. This was “face - to – face time with the patient and family. Although time is not taken into account as a factor for determining the level of E/M care for most medical encounters, timeis often the key or controlling factor in selecting the level of service in headache management. When counseling and Coordination of care is the CPT determining factor, there is no consideration of the extent of the history, the exam, the medical decision making required, or the nature of the presenting problem.