Download
1 / 22
380 likes | 1.25k Views
Disorders of the ankle and foot. Angela Hauksson Desember 2005. Ankle Anatomy. - Ankle Anatomy Muscle A P - Ankle Anatomy Muscle Posterior. Ankle Anatomy. Ankle Anatomy. Ankle Anatomy Function Flexion And Extension. Ankle Anatomy Ligaments. Ankle Anatomy.

E N D
Disorders of the ankle and foot Angela Hauksson Desember 2005
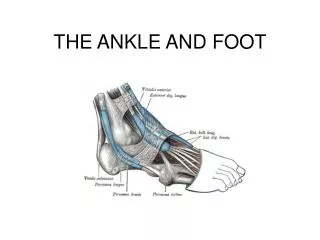
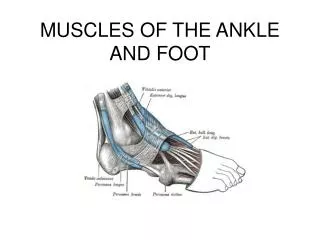
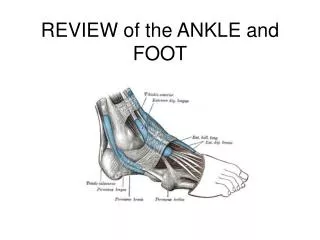
Ankle Anatomy - Ankle Anatomy Muscle A P - Ankle Anatomy Muscle Posterior
Ankle Anatomy Ankle Anatomy Function Flexion And Extension Ankle Anatomy Ligaments
Ankle Anatomy Ankle Anatomy Talar Intra-Articular Disorders Ankle Anatomy Subtalar Function
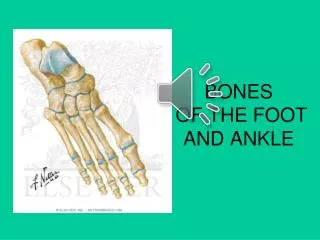
Foot Anatomy - Foot Anatomy Anterior - Foot Anatomy Joints
Osteoartritis of the ankle • can follow any damage of the joint ( fracture, repeated minor trauma, infecton) • dorsiflexion is usuallly the first to be affected • progrssively stiffer • painful to walk Footballer´s ankle • caused by repeated strains of the anterior capsule Treatment: • Conservative ( shoe, anti-inflammatory drugs) • Operative ( Excision of osteophytes from the neck of the talus and the anterior margin of the tibia; arthrodesis; Joint replacement )
Osteochondritis dissecant and osteochondral fractures • Traumatic defect in articular surface of talus • adolescence or young adulthood • small fragment of talus may separate from the body ( if the loose bodies are painful or cause mechanical symptoms they need to be removed, either arthroscopically or by arthrotomy). Aseptic necrosis of the body of the talus • fractures through its neck • Loss of height of the talus and a stiff ankle • progressively stiffer • becomes painless after a few years • no active treatment ( analgesics, firm boot to suppot the ankle )
Rheumatoid arthritis • The bone destructon produces a foot and ankle that are unstable, painful. • boneis lost => the ligaments no longer hold the bones in the correct position => the foot rolls into valgus and this in turn leads to a valgus deformity. Treatment: • Conservative ( ankle supports, surgical footwear) often ineffective • Operative: - arthrodesis usually effective - total ankle replacement - Osteotomy to correct the alignment
Ligamentous instability • recurrent episodes of minor instability • clinical and radiological examination are normal • most common site of injury are the lateral collateral ligament ( Posterior talofibular ligament, Calcaneofibular ligament, Anterior talofibular ligament) Treatment: • exercises to improve the postural reflex and strengthen the postural muscles around the ancle. • operation ( rerouting the peroneus brevis tendon or by a free graft of plantaris)
Subtalar joint • damage to the talus or fractues of the calcaneum can restrict eversion and inversion • difficlt or painful to walk over rough ground • commonly result from a fracture of calcaneum in a fall onto the heel • can take 2 years to reach their final state Treatment: • Until 2 years: firm boot to restrict inversion and eversion • After 2 years: subtalar fusion may be required
Midtarsal joinit • lies between the calcaneum proximally and the cuboid and navicular bones distally and with the tarsometatarsal joint • allows pronation and supination of the forefoot on the hindfoot. • subtalar, midtalar and tarsometatarsal joints are wery closely connected. – damage to one can impair the function of the other two. • trauma, talipes equinovarus, • painful restriction of movement in the foot Treatment: • conservative (firm shoe or boot) • triple fusion (antrodesis of all three joints) • pantalar arthrodesis (if the triple functon is accompanied by an ankle arthrodesis)
Köhler´s disease is an osteochondritis • self limiting avasulcar necrosis of the navicular; (unilateral, affects children age 4-5, most often boys) • The navicula is the last tarsal bone to ossify in children. Compression →ischemia →symptoms. • The child can walk with an increased weight on the lateral side of the foot; • pain tenderness, and swelling develop in the region of the navicular; • contraction of tibialis posterior muscle may be painful; Radiologic Findings: • navicular shows patchy areas of sclerosis, may appear collapsed, in some cases have normal shape • occassionally seen on opposite,asymptomatic foot Treatment: • symptomatic (pain and swelling) - soft longitundinal arch supporters, - limitation of strenuous activity; - if pain is severe - immobilize the foot in slight inversion for 4 to 6 weeks,(use of shoe modifications) Prognosis is excellent (normal ossification is usually completed in two years;
Sever´s disease (Calcaneal apophysitis) • in physically active growing children (girls 8 to 10 years old and boys 10 to 12 years old (often in boys). • pain in one or both heels with running and walking • The pain and inflammation is localized to the point of the heel where the heel cord (Achilles Tendonitis) inserts into the heel bone (Calcaneal apophysitis), and is tender to deep pressure at that site. • Walking on his toes relieves the pain • Biopsies of similar conditions have shown changes consistent with separation of the cartilage. The condition is very similar to Osgood-Schlatter’s disease which occurs at the knee. Treatment • non-steroidal anti-inflammatory medications • decreasing activity, boot in slight equines • the symptoms usually resolve within 12 months. • The condition is self-limited, however, it may take a prolonged period of time until it completely resolves.
Freiberg´s disease • Osteochondrosis of the head of the second and/or third metatarsal bone. • most frequently seen in the ages of 13-15 years. Females:males=3:1. • begins as a pain in the ball of a child's foot (result of a loss of blood flow to the growth plate in the bone) • the head of the metatarsal is palpable and tender • pain may persist for 1 or 2 years • On radiology the head of the metatarsal is shown to be wide and flat. Treatment • reducing pressure under the affected bone.( orthotic shoe) • If the discomfort is marked then the metatarsal head may be excised.
Accessory bones of the foot • 21 accessory bones of the foot have been discovered (includes the sesamoid bones) • 25% of the feet of adults and 22% of the feet of children under 16 years of age have roentgenographic evidence of one or more accessory bones. • Os trigonum – lokal pain (simptomatic treatment, excission) • Accessory Navicular bone – local tenderness from pressure of the shoe ( excision of bone and fixation of the posterior tibial tendon) Os vesalinum os peroneum Os Trigonum os tibiale externum Accessory Navicular
Plantar fascitis • an inflammatory condition affecting the fascia on the bottom of the foot • most common cause of heel pain. • stretches irregularly and develops small tears that cause the ligament to become inflamed. • common problem among middle-aged adults and some athletes (Shoes, work,running habits) • Pain on the sole of the foot (front of the heel) • Pain is worse in the morning; often aggravated by standing, walking or running. • Bone spurs are easily detected on x-rays. Treatment • early treatment is the most effective. • ultrasound, current, rest, ice massage, exercises to strengthen the plantar muscles, stiff boot, Soak with Epson salts will draw inflammation out of the sore muscles, night splints as the most beneficial treatments for heel pain. • ibuprofen cream, steroid injection ( painful and often ineffective). • excision ( fasciotomy) is usually ineffective.
Hallux rigidus“stiff big toe” • Painful loss of motion of the MTP joint of the great toe (result of osteoartitis) • An enlarged first MTP joint, which may be palpable on the skin • Dorsiflexion of the toe is markedly reduced, and painful, with a sensation of an abrupt bony block. • Pain with any walking ( elevated heel or hyperflexible sole increases the pain). • In the adolescent or middle aged ( previous trauma ) Treatment: • conservative (low-heeled shoes, a soft cushioned rubber sole, with a metal or fiberglass plate) • NSAIDs may be beneficial on a short-term basis. • Excision of the dorsal osteophytes and osteotomy of the proximal phalanx (sometimes helpful) • Excision arthroplast (Keller´s operation) is sometimes effective. • Arthrodesis is reliable. The toe should be fixed in slight dorsiflexion. • Interposition arthroplasty with a Silastic spacer
Hallux valgus • causes is unknown ( pointed shoes? High heels? Heredity?) • The hallux valgus angle is formed by the intersection of the longitudinal axes of the proximal phalanx and the first metatarsal. • Normal average deviation in adults - up to 15° • Mild hallux valgus - 15° - 20° angle • Moderate deformity - a hallux valgus angle 20° - 40° • Severe deformity - a hallux valgus angle of more than 40° • Two main groups: 1- adolescents and young adults (often familial), 2- elderly women, and occasionally men. Treatment • sponge pads and splints, surgical shoes. • operative. 1. metatarsal osteotomy – (younger patients) 2. Exostectomy 3. Excision arthroplasty (Keller´s operation) – (older) 4. Arthrodesis – (men)
Hammer toe (Digitus malleus) • deformity of the second, third or fourth toes. • the toe is bent at the middle joint (resembles a hammer) • People have corns or calluses on the top of the middle joint of the toe or on the tip of the toe, feel pain in their toes or feet and have difficulty finding comfortable shoes. • results from shoes that don't fit properly or a muscle imbalance Treatment • Conservative ( soft, roomy shoes; toe exercises; available straps, cushions or nonmedicated corn pads to relieve symptoms). • Operative: - Arthrodesis of the PIP joint (correct the deformity but only if the metatarsophalangeal joint is normal)
Metatarsalgia - pain in the forefoot • common cause - an inflammatory condition of the metatarsal heads of the foot - often a result of faulty distribution of weight on the forefoot (commonly occurs with women) - can follow any operation on the forefoot (Keller´s ). • burning sensation and pain in the area of the ball of the forefoot, often a dull ache, much like a bruise, often be localized to one metatarsal head. • Pain is located, on the underside of the foot but it may also radiate over the foot and sometimes up the calf - worse with walking barefoot, especially on hard surfaces like concrete or ceramic tile - less in good running shoes. Treatment: • Conservative ( ice on the ball of the foot, correct type of shoe ) • Operative ( metatarsal osteotomy).
Morton's Neuroma • is a fibrosis around the neurovascular bundle of the lateral and medial plantar nerves (between the third and fourth metatarsal heads) • mechanisms of injury: repetitive trauma, hammer or claw toes. • exhibits similar symptoms to Metatarsalgia, but may also cause numbness, tingling and discoloration of the third and fourth (lesser) toes. • The pain can be burning, sharp and agonizing, intermittent or constant. • neuralgia pain or numbness on the bottom of the foot, but out towards the toes. It starts on the ball of the foot and radiates out toward the 3rd and 4th toes Treatment: • Conservative (cold whirlpool, ultrasound; a metatarsal pad) • Surgical ( when conservative measures fail) - resection of the enlarged section of the nerve.