Download
1 / 38
380 likes | 530 Views
Analysis of Hospital Production: An Output Index Approach. Martin Gaynor Carnegie Mellon, NBER, CMPO Samuel A. Kleiner Carnegie Mellon William B. Vogt Rand and NBER Conference on Public Organisation Centre for Market and Public Organisation University of Bristol June 11-12, 2008.

E N D
Analysis of Hospital Production:An Output Index Approach Martin Gaynor Carnegie Mellon, NBER, CMPO Samuel A. Kleiner Carnegie Mellon William B. Vogt Rand and NBER Conference on Public Organisation Centre for Market and Public Organisation University of Bristol June 11-12, 2008
Hospital Costs and Policy Price regulation PbR (UK), Medicare, Medicaid (US),… Want price to reflect marginal costs Antitrust Merging parties normally claim efficiencies defense That is, economies of scale (possibly scope) Failing firm defense Planning Want to know scale, scope Specialty hospitals Are scope economies/diseconomies important? Are scale economies/diseconomies important? 2
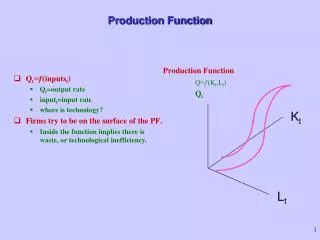
Hospital Costs and Economics • There are many outputs • Over 500 DRGs • Thousands of ICD codes • There is significant individual heterogeneity within outputs • Age, sex, race • Comorbidities, etc • Hospital have these characteristics in common with other service industries • Outputs difficult to pin down • “Mass-customization” • E.g., education, legal services, haircuts, … • Even “traditional” industries: electric power generation, steel manufacturing, shoes, brewing,... 3
Output Aggregation • Too many outputs to estimate econometric cost function with individual outputs • Curse of dimensionality • Need to aggregate • Economic Theory of Output Index • Ratios of marginal costs of aggregated outputs are independent of input prices (Hall, 1973) • Implies that outputs within an aggregation category should be similar with regard to input requirements
Previous Hospital Cost Studies • Most hospital studies are conducted using older data (1970s, 80s) • Technology has changed since previous studies • No firm conclusions as to the extent of scale economies and very limited evidence of scope economies • Scale Economies • Cowing and Holtman (1983), Vita (1990), Gaynor and Anderson (1995), Carey (1997), Dranove (1998), Hughes and McGuire (2003), Preyra and Pink (2006) • No Scale Economies • Grannemann et. al. (1986), Keeler and Ying (1996), Conrad and Strauss (1983), Fournier and Mitchell (1992) • Output typically defined as discharges or patient days, casemix variable added to function • Ad hoc • Clearly not consistent with requirements for aggregation • Preyra and Pink aggregate inpatient care into primary/secondary, tertiary 5
A Scale Economies Problem • Outputs captured in a crude way in previous work • It seems clear that more complex cases typically go to bigger hospitals • These two facts would seem to argue that scale economies are understated using conventional methods • Big hospitals look more expensive than they are due to more complex case mix
Research Objectives • Develop method for estimating hospital costs which: • takes account of hundreds of outputs • takes account of individual patient heterogeneity • attempts to aggregate in a way that’s consistent with economic theory • Use these methods to estimate hospital cost function with CA data • Use these methods to evaluate scale and scope economies & compare to more typical methods 7
Our Method vs. Previous • Previous literature uses crude output categories and adds an ad hoc casemix adjustment to take account of heterogeneity • We construct output indexes which build in output diversity and individual heterogeneity from the start • We estimate a long run cost function 8
Setup • Create 76 different hospital outputs • 25 MDC codes • Each with 3 levels of care (primary, secondary, tertiary) • Plus outpatient care • Each individual patient consumes his own individualized quantity of one of these 76 outputs • Outputs are aggregated upwards via output index
Setup, 2 Normal translog cost function with four aggregate outputs at the top level, primary, secondary, tertiary, outpatient Economies of scale, scope for these aggregate outputs estimated in the normal way, roughly Each top level output is an index of lower level outputs --- corresponding to the 25 MDCs ρ is a measure of scope economies within top-level outputs • ρ > 1: economies -- C(Y(Q1,Q2)) < C(Y(Q1, 0)) • ρ < 1: diseconomies -- C(Y(Q1,Q2)) > C(Y(Q1, 0)) 10
Setup, 3 • Each individual consumes a certain quantity of one of the outputs (primary, secondary, tertiary) • That quantity depends on his characteristics, qik= exp( Xikβk), k = P,S,T • Individual characteristics include DRG, age, sex, race, number of secondary procedures, number of secondary diagnoses, unscheduled admission • Accounts for individualized nature of hospital production
Setup, 4 • Then, each hospital’s level of each output is calculated by summing over the patients seeking care there: Iij is an indicator for patient i seeking care at hospital j In is an indicator for patient i’s diagnosis is in specialty n
Aggregate Output Classes • Classify inpatient output into four categories based upon input intensiveness • Primary Care: Inpatient illnesses which are least complex to treat • Secondary Care: Complex problems, specialist providers • Tertiary Care: Highly specialized providers, sophisticated equipment • Outpatient Care: Used hospital but not admitted as a registered bed patient • This classification is based on DRG • Rank DRGS based on: % of hospitals performing DRG, % of patients traveling for this DRG, % of procedures performed in teaching hospital, DRG weight • Top ranked 10% of discharges: tertiary • Next 40%: secondary • Lowest 50%: primary
Examples of Tertiary Care Nervous System • DRG 3: Craniotomy (brain surgery) • DRG 9: Spinal disorders & injuries Circulatory System • DRG 103: Heart transplant • DRG 107: Coronary bypass with cardiac catheter Newborn • DRG 386: Extreme immaturity or respiratory distress syndrome • DRG 387: Prematurity with major problems 14
Examples of Secondary Care Nervous System • DRG 20: Nervous system infection • DRG 10: Nervous system tumors with complications Circulatory System • DRG 130: Peripheral vascular disorders with complications • DRG 118: Pacemaker replacement Newborn • DRG 389: Full-term neonate with major problems • DRG 388: Premature delivery 15
Examples of Primary Care Nervous System • DRG 23: Nontraumatic stupor & coma • DRG 524: Transient ischemia (A neurological event with the signs and symptoms of a stroke, but which go away within a short period of time) Circulatory System • DRG 131: Peripheral vascular disorders without complications • DRG 134: Hypertension Newborn • DRG 391: Normal newborn 16
Estimating q • Motivation: To adjust for patient characteristics which relate to treatment intensity • Assume that hospital charges (Hijkn) can be expressed as: What we observe Change in cost for output type k at hospital j Change in output type k for additional unit of specialty n 17
Output Index • Taking logs and imposing qik= exp( Xik βk), we estimate the equation: where αjkn is a hospital-output type-specialty (MDC) specific fixed effect (321×3×25=24,075) X ik is a vector of observable consumer characteristics (# procedures, # diagnoses, age, etc.) βk is a vector of coefficients for these characteristics • Log quantity for individual i based on their observable characteristics: • Quantity for each hospital for output type k, specialty n is , and the quantity of inpatient output type k at hospital j is 18
Translog Cost Function with restrictions: • Second order approximation in logs to an arbitrary functional form with M inputs and K outputs (8 inputs, 4 outputs) • Shephard’s Lemma implies cost share equations can be written as: • Estimated using Nonlinear Seemingly Unrelated Regression 19
Estimation • The usual parameters of a translog cost function are estimated • In addition, ρ for each aggregate output must be estimated • Introduces significant nonlinearities to the estimation • In addition, β is estimated for each aggregate output category
Data • Data are from California’s Office of Statewide Health Planning and Development (OSHPD) for 2003 • Discharge Data • Contains information on patient demographic and diagnosis characteristics • 3.47 million observations out of 3.9 million • Include: • Individuals with data on total charges • Individuals from hospitals described below • Financial Data • Contains information on operating expenses, wages, ownership, facility size • 321 Hospitals • Exclude: • Specialty hospitals (long-term care, psychiatric, chemical dependency, children’s hospitals) • Hospitals not reporting data on charges (Kaiser & Shriner’s hospitals) 21
Variables • Costs: Total Operating Expenses • Inputs • Hourly wages for Nurses (RNs and LVNs), Technical Labor, Aides & Orderlies, Clerical Labor, Management • Equipment and Supplies • Capital price per bed [sq. ft.]*[construction cost]*[(int. rate) + (depr. rate)]/beds • Outputs: Primary Care, Secondary Care, Tertiary Care, Outpatient Care 22
Average Quantity Weights-Example • Quantity weights: 25
Diversification Parameter Estimates • Tertiary Care (ρt = 0.44 [0.35, 0.52]) - Implies diversification more expensive 19% savings to providing mean amount of tertiary care (989 discharges) in five MDCs versus ten • Secondary Care (ρs = 0.48 [0.37, 0.58]) - Implies diversification more expensive 8% savings to providing mean amount of secondary care (3,990 discharges) in five MDCs versus ten • Primary Care (ρp = 1.67 [0.44, 2.89]) - Implies diversification less expensive <1% savings to providing mean amount of primary care (5,129 discharges) in ten MDCs versus five 26
Economies of Scale • For multi-product firms, economies of scale calculated as where a value greater than 1 indicates economies of scale, less than 1 indicates diseconomies of scale. 28
Relative Performance of Output Index • Does the output index produce results different than would be produced using previous output definitions? • How do other studies define & classify output? • Total discharges or total patient days • Inpatient/outpatient • Append a “case mix” index which accounts for the relative severity of illness for a hospital’s Medicare population • Re-estimated the cost function • Classify output by inpatient/outpatient • Use discharge count while appending a case mix index 30
Economies of Scale-Comparison 155 beds 31
Economies of Scale-Comparison 180 beds 32
Economies of Scale-Comparison 220 beds 33
Economies of Scope • Is it cheaper to produce N products in N specialized firms or in one firm? • Are there savings from producing tertiary and secondary care together? How about primary and outpatient care? • Economies of Scope defined as: - Implies that the marginal cost of producing product i decreases with increases the amount of product j (weak cost complementarities) 35
Economies of Scope • Economies of Scope at the mean hospital ( ≈ 180 beds) between all care types 36
Summary and Conclusions • Output index shows diversification across MDCs may be cost increasing for tertiary and secondary care and cost decreasing for primary care • Output index produces estimates of scale economies higher than those recovered from typical methods • Economies of scope • Economies of scope between primary care and secondary care, as well as between primary care and outpatient care • Suggests potential for efficiencies (and thus possible benefits to consumers) even for large hospitals • This kind of method may be applicable to other industries. • Future work: panel data, instrumental variables, quality 37