Download
1 / 47
520 likes | 672 Views
Explore the mechanisms of myocardial blood flow alteration during stress, radiotracer comparison, imaging protocols, Tl-201 myocardial imaging process, patient preparation, and cardiac drug interference. Discover alternative stress testing methods and the quantitation process in MPS.

E N D
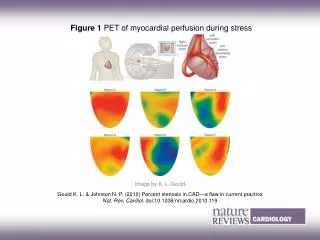
Physiological Alteration vs. Stress Chest pain ECG changes Regional dysfunction Diastolic dysfunction Molecular alteration Perfusion abnormality Stress Rest
Myocardial perfusion scintigraphy • Overview • Myocardial blood flow • 80-100 ml/min/100g at rest, 3-5 fold while demand • When tachycardia, absolute flow , but inner-to-outer flow ratio
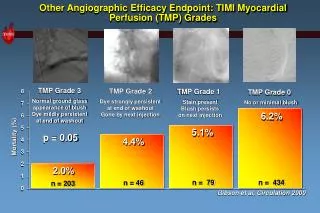
Myocardial perfusion Radiotracers • Mechanism, Extraction, and Linearity with flow
Comparison of MPS protocols • 201Tl stress-rest protocol • Long half-life, low dose, low count, poor spatial resolution, low energy, not well gated images, high scatter, attenuation • Stress always first • Probably optimal viability agent • 201Tl rest-redistribution protocol • Likely optimal and most cost-effective viability study • 99mTc sestamibi / tetrofosmin protocols • Better imaging characteristics, high resolution, least attenuation, no significant redistribution • Dual isotope 201Tl rest / 99mTc stress protocol • Brief with high throughput • 24-hr 201Tl imaging to maximize viability assessment • Difficulties in comparing 201Tl and 99mTc images
Tl-201 Myocardial imaging • Patient preparation: fasting for 4 hours. • Dosage: 2-3 mCi, i.v. • Stress imaging: 10 min post Tl-201 administration. • Rest imaging: 3-4 hr later.
Cardiac drugs that may interfere with stress testing and recommended withdrawal interval • Beta blockers 72 hr • Ca++ channel blockers 48-72 hr • Nitrates (long acting) 12 hr
Alternatives to leg exercise in cardiac stress testing • Isometric (handgrip) exercise • Atrial pacing • Esophageal pacing • Cold pressor testing • Ventricular stimulation; postextrasystolic potentiation • Pharmacologic stress