Download
1 / 14
160 likes | 968 Views
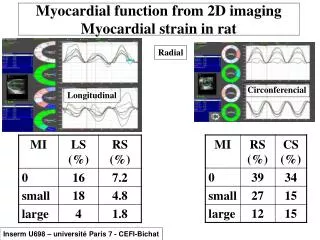
Prognostic Value of Myocardial Perfusion Imaging over Duke Treadmill Score. Ethan Levine, D.O., Regina S. Druz, M.D., FACC Department of Cardiology, State University of New York at Stony Brook and St. Francis Hospital Cardiac Imaging Research Group, Roslyn, New York.

E N D
Prognostic Value of Myocardial Perfusion Imaging over Duke Treadmill Score Ethan Levine, D.O., Regina S. Druz, M.D., FACC Department of Cardiology, State University of New York at Stony Brook and St. Francis Hospital Cardiac Imaging Research Group, Roslyn, New York
Case History (MC-10/2004) • 45 y/o non-diabetic, non-smoking male without personal or family history of CAD. • No medical care for the last 15 years • CC: exertional dyspnea for 1 month • Physical Exam: BP 130/100, HR 93 reg, resp 14 Cor: normal S1 and S2, no murmur Lungs: no adventitious sounds
Testing (MC-10/2004) • Pt. underwent treadmill exercise as follows: • Exercise Duration: 11:30 (Bruce protocol) • Reason for termination: dyspnea (onset @ 9 min) • Max HR 166 bpm (94% APMHR) • Max BP 170/100 mm Hg
ECG (MC-10/2004) • Rest: Sinus at 73 bpm, incomplete RBBB, otherwise unremarkable • Peak stress: Sinus at 166 bpm, 2mm ST depression in III, aVF; ST changes resolved 1 min into recovery
Exercise Data (MC-10/2004) • Patient’s Duke Treadmill Score • 11.5 – (5 x 2mm) – (4 X 0) = 1.5 • Correlates with 95% 4 year survival (moderate risk) 1 • Duke Score = Exercise Duration (min) – (5 X ST deviation (mm) ) – (4 x angina index) where angina index = 0 for none, 1 for non-limiting and 2 for limiting angina. • < -10 = High risk (81% four year survival) • - 10 - +4 = Moderate risk (95% four year survival) • > or = 5 Low risk (99% four year survival)
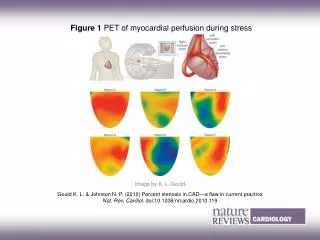
Imaging (MC-10/2004) • ADAC Cardio-60 dual-detector system • Raw data acquired over 180º orbit • Simultaneous gadolinium line source attenuation correction (VantagePro™, Milpitas, CA) • Iterative reconstruction • Gated 16-frame/cycle • Isotopes: Stress 30.9 mCi 99mTc sestamibi; rest 3.5 mCi 201Tl
Interpretation of Nuclear Data (MC-10/2004) • Large, severe intensity, reversible antero-septal and apical defect consistent with LAD ischemia (SSS=21) • TID suggestive of tight stenosis and/or multivessel disease • Gated Data: apical, septal and anterior severe hypokinesis. • Post Stress EF: 46%
Angiography (MC-10/2004) • 95% mid LAD lesion • (double click to play loop)
Angiography (MC-10/2004) • Trans-septal RCALAD collaterals • ( double click to play loop)
Discussion (MC-10/2004) • ACC/AHA guidelines recommend stress imaging in patients with an intermediate treadmill score to allow for further risk stratification, and guidance in patient management. • This case illustrates incremental benefit from myocardial perfusion imaging in patients with intermediate Duke treadmill score. The patient had HTN (unknown to him), but no other significant risk factors other than gender. His chief complaint was atypical (exertional dyspnea), and his exercise tolerance was very good. Overall, his pre-test probability of CAD was low-to- intermediate. Duke treadmill score put this patient at an intermediate risk for cardiac death and myocardial infarction. However, perfusion image data allowed further risk stratification into a high risk prognostic category. • This case illustrates that the extent of perfusion defects (SSS) and TID should be used together as markers of severe and/or multi-vessel CAD.
Teaching Points (MC-10/2004) • The Duke treadmill score is a useful measure of prognosis in outpatients with suspected CAD.1 • Duke Scores have been shown to be more predictive than clinical data, in risk stratification of patients with CAD. • The ACC advises imaging in patients with intermediate treadmill scores.2 • Patients with Intermediate treadmill scores and normal myocardial perfusion imaging studies have low event rates similar to the background population. However, severe perfusion defects in the setting of the same intermediate treadmill scores predict event rates approaching 11%.3
References • 1. Mark, DB, Shaw, Linds et al. Prognostic Value of A Treadmill Exercise Score in Outpatients With Suspected Coronary Artery Disease. N Engl J Med 1991; 325: 849-53. • 2. Gibbons R, Baladay G, Bricker JT et al. ACC/AHA 2002 Guideline Update for Exercise Testing: Summary Article. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1997 Exercise Testing Guidelines). Circulation 2002; 106: 1883-1892 • 3. Iskander, S and Iskandrian, AE Risk Assesment Using Single Proton Emission Computed Tomographic Technetium-99m Sestamibi Imaging. J Am Coll Cardiol1998;32: 57-62 • 4. Mazzanti Marco, Germano G et al. Identification of Severe and Extensive Coronary Artery Disease by Automatic Measurement of Transient Ischemic Dilation of the Left Ventricle in Dual – Isotope Perfusion SPECT. Journal of the American College of Cardiology. 27(7):1612-20, 1996 Jun