Download
1 / 23
250 likes | 343 Views
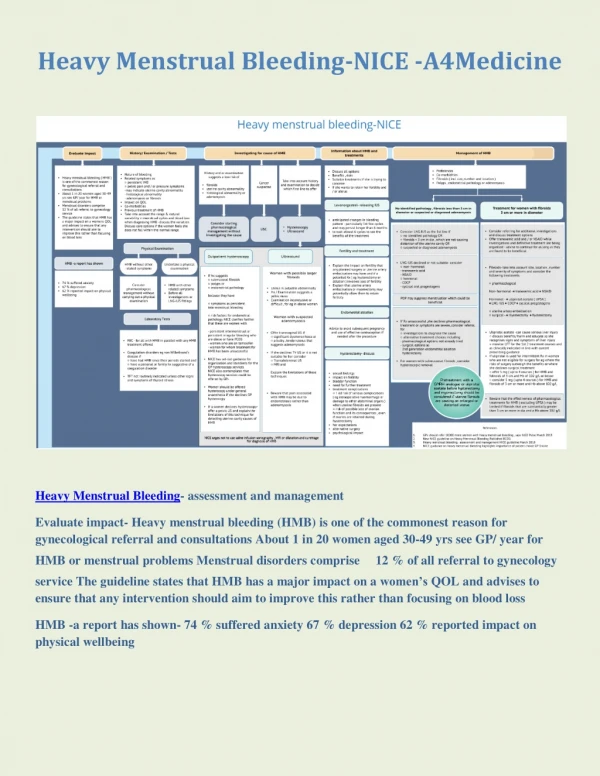
Learn about Heavy Menstrual Bleeding (HMB), its definitions, causes, and impact on women's quality of life. Discover history-taking tips, essential examinations, and laboratory tests in primary care.

E N D
Heavy Menstrual Bleeding Max Brinsmead PhD FRANZCOG September 2012
A Few Definitions • Menorrhagia • Excessive menstrual loss at regular intervals • Metrorrhagia • Excessive menstrual loss without evidence of any cycling • Typical of anovulatory bleeding at the extremes of reproductive life • Intermenstrual bleeding (IMB) • Episodes of bleeding between menstrual periods • Postcoital bleeding is a type of IMB • The generic modern terms are Heavy Menstrual Bleeding (HMB) & Abnormal Uterine Bleeding (AUB)
Heavy menstrual bleeding is defined as: • Excessive menstrual blood loss which interferes with a woman’s… • physical • emotional • social or • material quality of life • This implies that the woman herself is the primary judge of severity • And there can be substantial variation in tolerance to this dis - ease
While a pathological description is impractical: • That is, the menstrual loss of an amount of blood loss that is likely to lead to health sequelae • Because treatment options have risk & cost implications, a health provider is obliged to indicate to patients some criteria for diagnosis • My criteria: • Sufficient to cause iron deficiency (exclude other causes) • Escapes from accepted menstrual protection • Requires changes > 4 hourly • Up at night more than once • Passage of large clots • Lasts for >7 days (full flow)
Incidence of Heavy Menstrual BleedingThe Impact on Women • Cross sectional studies indicate that 5 – 50% of women will complain of “heavy periods” • Quantified studies show that ≈ 10% of women will have menstrual losses that ≥ 80 ml • Many studies indicate that the condition is associated with… • Reduced employment options • Work absences • Decreased earning capacity that for women are more important than such psychological effects as… • Depression and anxiety • Mood changes, irritability • As well as effects on social life, hobbies etc • Can be summarised in “Quality of Life” measures
Some Causes of Heavy Menstrual Bleeding • Fibroids • Adenomyosis • Endometriosis & Chronic PID • Endometrial cancer • Bleeding disorders • Idiopathic and acquired thrombocytopenia • Other known & undiagnosable disorders of coagulation • Physiological • Includes dysfunctional uterine bleeding • All studies show >50% have no identified pathology
Some History-taking Tips • How many days does your period last for • How many heavy days? What do you mean by heavy • What do you use for menstrual protection • How often do you change? Why do you change so often • What do you use at night • Do you change at night? How many nights • Do you pass clots? How big are the clots? How often • Any accidents (escape from menstrual protection) • What do you mean by flooding • Do you have to modify your life when you have your periods • What do you do for contraception in your relationship • Do you experience any other bleeding or bruising • Are you taking iron tablets
Other History-taking Essentials • Consider the cultural context • Explore parity, fertility requirements etc • Consider occupation and activities • The extent of examination and investigations will depend on • Age >45 • Intermenstrual bleeding • Any pelvic pain or pressure symptoms • Details of any previous gynaecological interventions • Other illnesses or conditions may influence treatment options • Other symptoms may influence treatment choices • Infertility • Prolapse • Urinary incontinence • Family History
Examination • A general examination of all patients • Height & weight • Signs of anaemia • Signs of endocrinopathy • Thyroid • Androgen excess • Abdominal examination • For significant uterine enlargement • Only rewarding in slim patients • A palpable uterus is >12w size • A vaginal examination is not required in primary care if there is no palpable uterus & a Pap smear is not required • Unless a Mirena is planned • And patients should not be sent for US without prior VE
Laboratory Tests in Primary Care • A Full Blood Count (FBC) for all patients • Look for iron-deficiency anaemia • Check the platelet count • S Ferritin • Is the most sensitive indicator of Iron deficiency • But it is an acute phase reactant • Thyroid function tests • Only when clinically indicated • Female hormones • Have no role • Even when the diagnosis is dysfunctional uterine bleeding
Indications for Tests of Coagulation Disorders • Symptoms from menarche • Positive Family History • Other personal bleeding or bruising • There is thrombocytopenia • Tests to do: • Renal and Liver Function Tests • Bleeding time and Coagulation time • Seek specialist haematological advice • The most commonly identified abnormality is von Willebrands Disease
Imaging in Primary Care • Ultrasound is the imaging of choice • But is not required unless the uterus is enlarged • Required for uncertainty after pelvic examination • Required after a failure of primary medical treatment • Required information from this examination include: • Uterine size including length of the endometrial cavity • Myometrial abnormalities • Any adnexal pathology • Considerable caution is required when... • Comments about endometrial thickness are reported as abnormal • Fibroids <4 cm in size are reported • Multiple fibroids are reported but there is no clinical evidence of an irregular uterus • Adnexal cysts <5 cm diameter are reported
What is the risk of significant pathology? • This is mostly about the risk of endometrial cancer • There are many studies… • Most do not distinguish between HMB and AUB • The risk of endometrial Ca is age dependent • For women <30 yrs age the risk is 1:10,000 • For those >45 years the risk is 8:10,000 • And the risk of endometrial hyperplasia is ≈ 4X higher • Who is at risk of Endometrial Cancer? • Those with intermenstrual bleeding • Those with irregular cycles – PCO disorder • Infertility • Obesity • Positive Family History
Indications for Referral • Patient is >45 years of age • There is irregular or intermenstrual bleeding • The uterus is >10 weeks size • There are symptoms or signs suggestive of such pelvic conditions as endometriosis, PID , adnexal pathology etc. • Ultrasound suggests uterine fibroids >4 cm or distortion of the uterine cavity • Failure of primary pharmaceutical treatment • Patient request
Medical Options for the Treatment of Heavy Menstrual Bleeding • Hormonal • Levonorgestrel IUS (“Mirena”) • Combined COC • Cyclical oral Progestins • Injected Progestin (“Depo Provra”) • Danazol • GnRH analogues • Non Hormonal • NSAIDs • Tranexamic Acid (“Cyclokapron”)
Surgical Treatment Options for Heavy Menstrual Bleeding • Endometrial Ablation • Hysteroscopic endometrial resection • 2nd generation techniques • Thermal balloon endometrial ablation (TBEA) • Microwave endometrial ablation (MEA) • Myomectomy • Uterine Artery Embolisation • Hysterectomy • Abdominal, vaginal or laparoscopic • Subtotal or total • With or without bilateral oophorectomy
The Mirena IUS for HMB • Reduces mean menstrual loss by 71 – 96% • Up to 50% of patients amenorrhoeic after 6m depending on age • ≈ 85% patients are satisfied (continuation rate) • ≈ 1% rate of troublesome hormonal side effects • When compared to endometrial ablation (EA) • Mean reduction in blood loss is greater with EA • But overall satisfaction equal • And Mirena better in the longer term (1 small study) • When compared to hysterectomy • Overall satisfaction rates are equal • But Mirena is half the cost even when up to 40% of patients go on to hysterectomy
Oral Hormones for HMBWhat is the Evidence? • Mean blood loss (MBL) is reduced by ≈40% • Risks in older women and smokers plus side effects limit use of COC (oestrogen) • Progestin e.g. Norethisterone 5 mg TDS from Day 5 to 27 of a cycle is effective in reducing (MBL) • Progestin not as effective as NSAIDs and Tranexamic acid • Side effects are limiting – weight gain, headaches, acne, mood changes, mastalgia • They are of most use in the short term treatment of DUB at the extremes of reproductive life
IM Depo Provera for HMB • ≈10% of patients are amenorrhoic after 3m of 150 mg every 12w • ≈50% amenorrhoic after 12m • Continuation rates are low, however, presumably due to side effects • And there is a small risk of bone mineral loss with long term use
GnRH analogues for HMB • Most studies have been directed at the reduction of uterine size with these agents that induce a “reversible menopause” • Reductions in uterine size up to 75% over 6m can occur • And up to 90% of patients achieve amenorrhea • This can be very useful prior to hysterectomy • Oestrogen-deficiency symptoms i.e. hot flushes, vaginal atrophy and bone loss are limiting • But these can be overcome with add-back therepy using small doses of oral oestrogen, COC, progestin or tibilone • GnRH are currently very expensive drugs
Tranexamic Acid (Cyklokapron) for HMB • Inhibits plasminogen activation but has no effect on blood clotting in healthy vessels • Reduces fibrin breakdown in spiral arterioles • Systematic reviews confirm that mean blood loss during menstruation is reduced by ≈ 50% • 12% of women experience side effects • Nausea, vomiting, dyspepsia • Diarrhoea • No apparent risk of thromboembolism • Visual side effects are rare • Dose 1G every 6 – 8 hours • It is not contraceptive nor cycle regulating
NSAIDs for HMB • Systematic reviews confirm that mean menstrual blood loss during menstruation is reduced by ≈ 30% • Mefanamic acid e.g. Naprosyn better than Ibufren e.g. Indocid • Side effects are well known but risk is reduced by intermittent use • Dose 1 – 2 tablets 4 – 6 hourly • Particularly useful when dysmenorrhoea is also a problem • Not recommended if there is a known bleeding disorder loss
Information for Patients that compares Endometrial Ablation & Hysterectomy