Download
1 / 36
370 likes | 513 Views
Detailed guide on anesthesia considerations for posterior fossa surgery, case approach, complications, and monitoring techniques. Learn about sitting position advantages, complications, and contraindications.

E N D
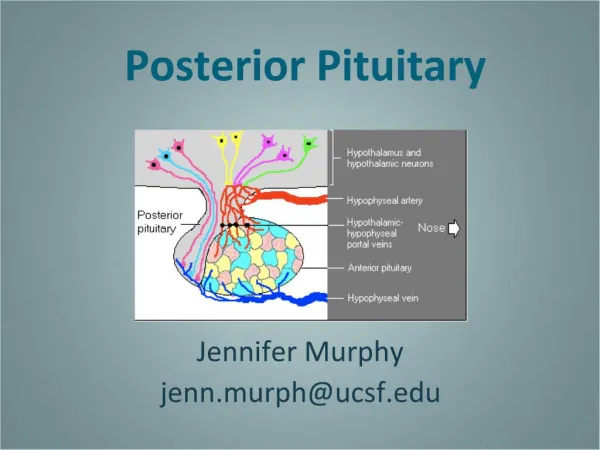
Posterior Fossa Procedures(Infratentorial Craniotomy)and Neuroanesthesia Emergencies Mani K.C Vindhya M.D Asst Prof of Anesthesiology Nova Southeastern University
Anesthesia forPosterior Fossa Procedures(Infratentorial Craniotomy)and Neuroanesthesia Emergencies • I. Format = approach to posterior fossa case • Preoperative concerns – • Problem list? • Further labs and studies? • Optimization? (Is the patient optimal for surgery?) • Consults? • Further medical treatment? • Intraoperative concerns • Premedication • Monitoring • Induction • Maintenance • Intra-op complications (2 main complications?) • Emergence • Postoperative concerns – only on the long stem • 2 main complications? • Post-op pain relief
Posterior fossa considerations • Case Presentation. • An 18 year-old male for posterior fossa exploration and excision of cerebellar mass lesion. History • headache • nausea and vomiting • impaired hearing • occasional diplopia Physical exam • ataxia • severe bilateral papilledema (3/4) • BP = 120/70 to 140/80 • weight = 65 kg CT scan • cerebellar mass lesion • hydrocephalus The neurosurgeon desires intraoperative monitoring of: • brain stem auditory evoked potentials (BAEP's) • facial nerve (cranial nerve VII) function
Problem List: • Cerebellar mass lesion with hydrocephalus • Increased ICP • Positioning -- sitting, prone, lateral, or supine (semi-lateral) • "Full stomach" -- nausea and vomiting, increased ICP • Intraoperative monitoring • Brainstem auditory evoked potentials • Facial nerve function (motor testing)
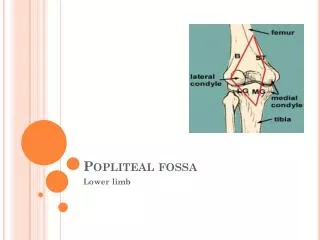
Posterior Fossa • Is a "closed-in" space • Bone - on sides, back, and bottom • Tentorium - on top (Posterior fossa is "infratentorial.") • Brain stem - in front • Contains about 1/4 of intracranial contents • Tumors in the posterior fossa • Children • Intracranial neoplasms = the most common solid tumors in • childhood (about 25% of all admissions for neoplastic disease). • Posterior fossa = the site of origin of 50 to 60% of brain tumors in children. • Adults -- uncommon site for brain tumors • Tumors in the posterior fossa are often: • "Benign by histology" • "Malignant by location" • Posterior fossa tumors can compress the brain stem (pons and medulla). • CSF outflow tracts • Cardiovascular centers • Respiratory centers -- pneumotaxic center, apneustic center
Sitting Position • Situations in which sitting position might be used are mainly: • Posterior fossa procedures • Cervical laminectomy • Establish which position the surgeon desires for posterior fossa surgery: • Sitting • Prone • Lateral decubitus • Supine (semi-lateral) • Proper positioning for a seated posterior fossa operation • Knees at heart level Neck not hyperflexed
Advantages of the sitting position include: • Excellent surgical access • Comfort for the surgeon • Facilitates hemostasis (decreased blood loss) • Improved venous and CSF drainage • Exposes face for monitoring response to cranial nerve stimulation (though this can also be done electronically)
Possible sitting position complications include: • Air embolism (venous and arterial) • Cardiovascular instability • Hypotension • Venous pooling • Cardiac arrhythmias • Neurologic complications • Quadriplegia • Nerve injuries (e.g. ulnar, sciatic, lateral peroneal) • Pneumocephalus • Airway obstruction • Airway swelling (head and tongue) • Malpractice risk. The use of the sitting position for posterior fossa neurosurgery is somewhat controversial. • Current practice is away from operating in sitting position6 • No evidence that position affects outcome. • Venous air emboli can occur in any position -- • sitting, lateral, prone, or supine
Relative Contraindications to Sitting Position • Known cardiac septal defect = a "red flag" • Patent foramen ovale (PFO) • Atrial septal defect • Ventricular septal defect • Right atrial pressure > left atrial pressure • Functioning ventriculo-atrial shunt • ?? cardiac instability • ?? extremes of age
Air Emboli (Venous and Arterial) • Incidence of venous air emboli (VAE) can be as high as 50% in neurosurgery. • Incidence of VAE depends on both monitoring and position.10 • "Bottom line" on VAE: • More frequent in the sitting position. • BUT -- VAE can occur in any position. • Early detection and prevention with the Doppler and other more sensitive • VAE monitoring methods have: • Decreased the occurrence of clinically significant VAE • Increased the reported incidence of VAE
Comments on VAE monitors • Bubble Doppler -- still a very sensitive and practical way to detect VAE • Transesophageal ECHO (TEE) • The most sensitive way to detect VAE. • The only way to document intraoperative "paradoxical air emboli" which have crossed to the arterial circulation, unless the surgeon sees air bubbles in arteries! • ECHO could be used to detect a patent foramen ovale preop. • Incidence of patent foramen ovale = about 1 in 4. • A paradoxical air embolus can occur even if a person does not have a patent foramen ovale. Air can traverse the pulmonary circulation. • Why don't we get pre-op ECHO's for all sitting position cases? • Expensive • The number of complications as a result of paradoxical air emboli is actually small
Pulmonary artery pressures (PAP) • CVP catheters: • Have two uses regarding VAE: • VAE detection (much less sensitive than Doppler or TEE) • VAE aspiration (potentially life-saving in some situations) • How do you confirm CVP catheter placement in the right atrium (to aspirate air lock if VAE occurs)? • Length of catheter (but could be in jugular vein) • Rapid saline bolus through CVP (listen to Doppler) • PAC's (imply atrial stimulation) • PVC's (imply ventricular stimulation) • Right ventricular pressure wave on CVP (Pull catheter back into right atrium.) • Chest X-ray • Biphasic P-wave on intracardiac electrocardiogram
Intraoperative Concerns • Premedication? • Thorough pre-op interview to allay anxiety. • None ("light" sedation with benzodiazepine if at all). • Avoid narcotics pre-op (respiratory depression, nausea and vomiting). • Monitoring Checklist -- use "routine" monitors as reminders: • Stethoscope -- esophageal • Precordial Doppler -- to detect venous air emboli (VAE) • EKG -- ST segments • Non-invasive blood pressure • Radial A-line -- BP, paO2, paCO2 (=25-30), H&H, K+ • CVP -- follow volume status, aspirate VAE • Temperature -- esophageal probe • Blood warmer, Bird or Bear humidifer • Warming/cooling blanket
Oxygen monitor (+ volume monitor and PIP) • Adjust ventilation according to paCO2 • Pulse oximeter • End-tidal CO2 (and infrared gas analyzer) • Useful to trend paCO2 (End-tidal CO2 < paCO2) • Detecting VAE (decreased end-tidal CO2, increased ET N2) • Restraints (+ twitch monitor -- muscle relaxants) • Intake and output • Foley catheter (furosemide, mannitol) • Maintain even I&O (Don't "run em' dry.") • Avoid dextrose-containing solutions in IV's • Position injuries • Ulnar or sciatic nerves (in sitting position) • Neck not hyper-flexed or -extended
Special monitors 1. Facial nerve (C.N. VII) function • Neurosurgeon directly stimulates facial nerve in operative field. • Facial muscle movement is observed: • Directly by the anesthesiologist (under drapes) • Indirectly by electrode and monitor • Anesthetic implication -- neuromuscular blockade must wear off or be reversed at time of stimulation. 2. Brainstem auditory evoked potentials or responses • (BAEP's or BAER’s) • Specialized form of EEG monitoring • Background EEG activity is electronically subtracted out. • The EEG waveform evoked by auditory stimulus (clicking in ear) remains.
Shape of a typical BAEP = seven peaks1 • Latency = time to first peak (usually 2 msec) • Amplitude = height of the peaks c. The seven peaks of the BAEP are believed to correspond to passage of a stimulus through "generators" in the auditory nerve, brainstem and cortex.
What do we look for during surgery? • Mainly two things: • Increase in latency (> 10%) • Decrease in amplitude (<50%) • These two changes could be indicative of impending injury or ischemia in the BAEP pathway. • BAER's are barely affected by anesthetics: • No anesthetic drug produces a change in BAER’s that • could be mistaken for a surgically induced change. • 2) Etomidate decreases amplitude and increases latency (but this is not clinically significant).
Induction -- "typical" anesthetic regimen for intracranial procedures,assuming airway meets good criteria (i.e. Mallampati classification): • 1. Method: "Modified" rapid sequence induction and intubation (with cricoid pressure) • Preoxygenate and denitrogenate (100% O2 by mask with head in good "sniffing" position) • Cricoid pressure (N&V with increased ICP) • Hyperventilate to decrease paCO2 prior to intubation • Typical induction agents • Propofol, etomidate, or thiopental • suitable I.V. induction agents • Fentanyl or sufentanil – as narcotic analgesics to supplement • Lidocaine IV – to blunt hypertensive and ICP response to intubation d. • Neuromuscular junction blockers –rocuronium, vecuronium, or succinylcholine (with prior defasciculating dose of non-depolarizing NMJ blocker)
Maintenance • 1. Reasonable Maintenance Regimens for Intracranial Neuroanesthesia (going from routine to desperate). a. N2O + isoflurane (½%) + fentanyl • N2O = the first agent to go if there’s brain swelling or venous air emboli or ischemia danger (i.e. aneurysm or head trauma) • MAC equivalents of sevoflurane or desflurane might also be substituted for isoflurane. • Sufentanil could be substituted for fentanyl. b. Isoflurane (1%) + fentanyl c. Isoflurane (½%) + propofol + fentanyl • ! Volatile agents are next to go if high ICP or brain swelling • Total IV anesthetic: Propofol + fentanyl • Barbiturate coma -- for intractible brain swelling or cerebral • protection during aneurysm clipping (titrated to EEG burst suppression): • Thiopental • Pentobarbital
Non-depolarizing neuromuscular junction blocker (must wear off or be reversible by time of CN VII testing). • Vecuronium • Rocuronium • Pancuronium – increases HR • Cis-atracurium • Additional maneuvers to decrease ICP
Intraoperative Complications -- "Emergencies in Neuroanesthesia" • Intraoperative Air Embolus • What should I do immediately? • Tell the surgeon, who should flood the field. • Discontinue N2O and give 100% O2 • Aspirate air from the CVP line • Light neck compression • Call for help • Supportive measures (i.e., treat hypotension, arrhythmias) • Try to position patient for CPR • What else can I do? Other considerations: • Dopamine or dobutamine? (Suggested to increase right ventricular contractility) • Raise CVP by fluid loading, not PEEP. PEEP would raise CVP, but at the risk of sending a paradoxical (arterial) air embolus through a probe-patent foramen ovale. • Avoid the Valsalva maneuver:This increases CVP, but: • could cause paradoxical air embolus • causes severe hypotension
"Tight Brain" -- Think through things we can do to decreaseintracranial volume and ICP. • Airway disaster? In any anesthetic emergency, the first things to think of are: HYPOXIA & HYPERCARBIA! (Is this a respiratory disaster?) • Furosemide and mannitol? • Dexamethasone? • Open the spinal drain or insert a ventriculostomy? • Can I hyperventilate more (to paCO2 of 25)? • Anesthetic choice? • Muscle relaxant? • DC N2O, switch to 100% O2? • TIVA (total IV anesthetic) technique? • Barbiturate coma – as a last resort • Improve venous return? • Reverse Trendelenberg position? Elevate head of bed? • Reposition the head? Is there venous occlusion secondary to positioning?
Sudden Cardiovascular Changes a. With any sudden change in vital signs (hyper- or hypotension, tachy- or bradycardia, cardiac arrhythmias, etc.), the first three things to think of in this situation are: • HYPOXIA & HYPERCARBIA! (Always first) • SEVERE AIR EMBOLUS (Close second) • Artifact - has BP transducer or table moved up or down? b. Bradycardia 1)With hypertension a) Most likely cause = Cushing response 2ndary to: • ICP (closed skull) • surgical retraction (open skull) • brain stem stimulation • traction on trigeminal nerve (CN V)
Potential treatments: • Tell surgeon. • Propofol or pentothal bolus • Deepen anesthesia • Other possible causes: • Impending brain stem herniation (turn off spinal drain?) • Inadvertent phenylephrine bolus • Bradycardia With hypotension • Most likely cause = vagal stimulation • Potential treatments: • Tell surgeon. • Ephedrine • Atropine (or glycopyrrolate)
Tachycardia • With hypertension • Most likely causes = light anesthesia or sympathetic stimulation • Another cause = inadvertent Ephedrine bolus • Potential treatments = deepen anesthesia (1st), antihypertensives (2nd) • With hypotension • Most likely cause = hypovolemia • Another cause = hemodynamic instability due to sitting position • Potential treatments: • Replace I&O cc per cc • Phenylephrine
Emergence. • Hypertension is frequently a problem. • Avoid "coughing and bucking" while head is secured. Two agents to treat coughing and bucking are: • Propofol • Lidocaine • It's desirable for the patient to awaken quickly so neurosurgeons can obtain a neurologic assessment.
Postoperative Concerns. • Many potential postoperative problems are relatedto the location of the surgery on or near the brain stem. • Cardiovascular centers - hypertension • Respiratory centers - respiratory depression, apnea • Lower cranial nerves: