Craniotomy
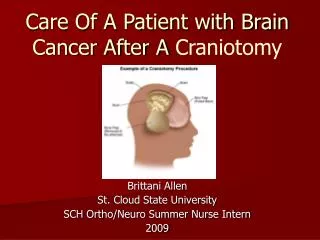
Craniotomy. Craniotomy. craniotomy is a surgical opening of the skull to gain access to portion of the CNS inside the cranium. Cases that craniotomy is required :- Brain tumor resection or removal. cerebral decompression. evacuation of hematoma or abscess.

Craniotomy
E N D
Presentation Transcript
Craniotomy • craniotomy is a surgical opening of the skull to gain access to portion of the CNS inside the cranium. • Cases that craniotomy is required:- • Brain tumor resection or removal. • cerebral decompression. • evacuation of hematoma or abscess. • clipping of aneurysm or removal of arteriovenous malformation.
Preoperative care * protection of the integrity of the CNS is the major priority of care for the patient awaiting a craniotomy. * detailed assessment and documentation of the patient’s preoperative neurological status are imperative for accurate post operative evaluation. * in pituitary patient, evaluation of endocrine function is necessary to prevent intraoperative and postoperative complication. * routine preoperative screening should be performed( CBC, BUN, Cr, FBS, chest x- ray, ECG, cross match).
preoperative teaching is important to both patient and family about post operative period, which include the following issues:- • patient should know that all or part of his/her head’s hair will be shaved to do operation, patient should know about facial odema or periorbital ecchymosis, also patients should know about the suspected complication such as infection, hemorrhage, anesthesia problems, and also suspected neurological deficit. patient undergoing transsphenoidal approach requires preparation for the sensation associated with nasal pack.
Postoperative medical management • I- Intracranial hypertension: • Postoperative cerebral edema is expected to peak in the first 48 to 72 hours. Monitoring of the surgical site for herniation because of high ICP in the absence of bone flap. • Treatment include: CSF drainage, patient positioning by elevation of bed up to 30 degree, and steroid administration( dexamethasone).
II- surgical hemorrhage:- Manifested when there is neurological deficit or deterioration in the level of consciousness, which need re-exploration of the surgical site. III- fluid imbalance: • Observe for signs of diabetes insipidus( D.I):- • 1- polyurea: urine output more that 200 ml per hour. 2- Urine specific of 1.0005or less with elevation of serum osmolality and decrease in urine osmolality. • Observe for signs of SIADH
IV- CSF leak:- • Management of CSF leak:- head elevation, bed rest , suturing at the site of leak if possible and compressing dressing, taking sample from leakage for analysis if it is serous or CSF, or lumbar puncture or insertion of lumbar subarachnoid drain to drain CSF until dura heal.
V- deep vein thrombosis:- • DVT occur in 29% to 46% of all neurosurgical patient, as compared with 25% incidence in general surgical patients. Causes include: • operation lasted more than 4 hours • patient with supratentorial approach. • preoperative legs weakness. long stay postoperative in bed rest.
Postoperative nursing management Preserving adequate cerebral perfusion; 1- positioning( head elevation). 2- fluid management . 3- vomiting and fever. • Promoting arterial oxygenation
Providing comfort and emotional support : • control of headache. • administer stool softners and provide bowel program. • Maintaining surveillance for complication:- • infection. • corneal abrasions. • injury and convulsion.
Patient education. Initiating early rehabilitation