Download
1 / 35
410 likes | 1.11k Views
Premenstrual syndrome Dysmenorrhea. Dr.Roaa H. Gadeer MD. PMS/PMDD. The presence of physical and/or behavioral symptoms that occur repetitively in the second half of the menstrual cycle and often the first few days of menses. Incidence. 70 - 80% Only 20% are clinically significant.

E N D
Premenstrual syndromeDysmenorrhea Dr.Roaa H. Gadeer MD
PMS/PMDD • The presence of physical and/or behavioral symptoms that occur repetitively in the second half of the menstrual cycle and often the first few days of menses.
Incidence • 70 - 80% • Only 20% are clinically significant. • PMDD affect only 5-6% • Relatively high rates: Mediterranean countries, the Middle East, Iceland, Kenya, and New Zealand
Premenstrual syndrome : 1. The presence by self report of at least one of the following: somatic and affective symptoms during the five days prior to menses in each of the three menstrual cycles: Affective: Depression, Angry, outbursts, Irritability Confusion, Social withdrawal, Fatigue. Somatic: Breast tenderness, Abdominal bloating ,Headache, Swollen extremities. 2. Relief of the above symptoms within four days of the onset of menses, without recurrence until at least cycle day 13.
3.The symptoms are present in the absence of any pharmacologic therapy, hormone , drug or alcohol use. 4. Identifiable dysfunction in social or economic performance by one of the following criteria: • Marital or relationship discord. • Difficulties in parenting. • Poor work or school performance. • Tiredness/Increased social isolation. • Legal difficulties. • Suicidal ideation. • Seeking medical attention for a somatic symptom.
PATHOGENESIS • interaction of cyclic changes in ovarian steroids with central neurotransmitters. • Serotonin. • Beta-endorphin. • Gamma-aminobutyric acid (GABA). • Autonomic nervous system. • Peripheral mechanisms.
Symptom: • Fatigue 92 • Irritability 91 • Bloating 90 • Anxiety/tension 89 • Breast tenderness 85 • Mood liability 81 • Depression 80 • Food cravings 78 • Acne 71 • Increased appetite 70 • Over sensitivity 69 • Swelling 67 • Expressed anger 67 • Crying easily 65 • Feeling of isolation 65 • Headache 60 • Forgetfulness 56 • Gastrointestinal symptoms 48 • Poor concentration 47 • Hot flashes 18 • Heart palpitations 14 • Dizziness14
Diagnostic criteria are: • The American Psychiatric Association DSM-IV criteria for PMDD • The University of California, San Diego (UCSD) criteria for PMS
DSM-IV criteria (PMDD) : • Documentation of physical and behavioral symptoms being present for most of the preceding year. • Five or more of the following symptoms must have been present during the week prior to menses. • Resolving within a few days after menses starts. • At least one of the five symptoms must be one of the first four on this list: • Feeling sad, hopeless, or self- deprecating • Feeling tense, anxious • Marked liability of mood / tearfulness • Persistent irritability, anger, and increased interpersonal conflicts • Decreased interest in usual activities / withdrawal from social relationships • Difficulty concentrating • Feeling fatigued, lethargic, or lacking in energy • Marked changes in appetite, which may be associated with binge eating or craving certain foods • Hypersomnia or insomnia • Being overwhelmed or out of control • Breast tenderness or swelling, headaches, joint or muscle pain, a sensation of bloating, weight gain
UCSD criteria (PMS): • In whom coexisting medical conditions or psychiatric disturbance were excluded by history, physical examination and psychometric testing. • The presence of at least one of the following six Behavioral symptoms: - Fatigue, irritability, depression, expressed anger, poor concentration, and social withdrawal. • at least one of the following four Somatic symptoms: - Breast tenderness, abdominal bloating, headache, or swollen extremities
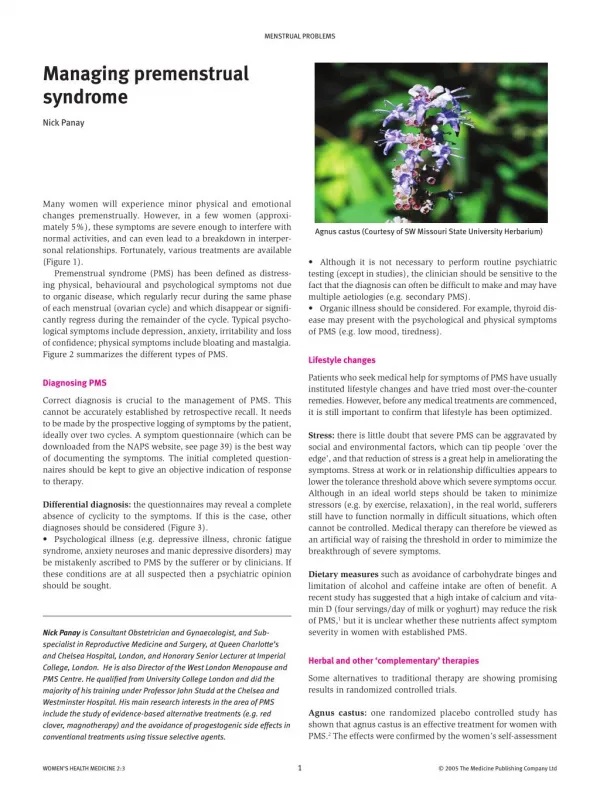
Therapies for the premenstrual syndrome Treatments with demonstrated efficacy: • Serotonin reuptake inhibitors (NOT Anti depressant) • Alprazolam • Agents that suppress ovulation • GnRH agonists • Danazol Treatments with possible efficacy • Oral contraceptives • Diuretics • Exercise Ineffective treatments • Progesterone • Vitamin supplements/Dietary restrictions
Dysmenorrhea: painful menstruation. • Primary Dysmenorrhea (PD): The presence of recurrent, crampy, lower abdominal pain that occurs during menses in the absence of demonstrable pelvic disease. • Secondary Dysmenorrhea: The occurrence of painful menstruation in the presence of a pelvic pathology, such as endometriosis, adenomyosis, uterine leiomyomata, or chronic pelvic inflammatory disease
Incidence • PD typically begins during adolescence • Not until ovulatory menstrual cycles are established. • At two years postmenarche (18 to 45%) teens have ovulatory cycles. • 80 % are ovulatory by four to five years postmenarche. • The prevalence of dysmenorrhea among adolescent females ranges from 60 to 93 percent, but decreases with advancing age
RISK FACTORS • Presentation at age less than 30 years. • Body mass index less than 20. • Menarche before age 12. • Longer cycles/duration of bleeding. • Irregular or heavy menstrual flow. • Premenstrual symptoms. • Pelvic inflammatory disease. • Sterilization. • History of sexual assault. • Heavy smoking.
Reduced risk of dysmenorrhea in: • Use of oral contraceptives. • Fish intake. • Physical exercise. • Being married or in a stable relationship. • Higher parity.
Major causes of secondary dysmenorrhea Gynecologic disorders • Endometriosis • Adenomyosis • Ovarian cysts • Pelvic adhesions • Pelvic inflammatory disease • Uterine polyps • Congenital obstructive müllerian malformations • Cervical stenosis Nongynecologic disorders • Inflammatory bowel disease • Irritable bowel syndrome • Uteropelvic junction obstruction • Psychogenic disorders
PATHOGENESIS • PD is caused by frequent and prolonged uterine contractions that decrease blood flow to the myometrium resulting in ischemia (uterine "angina"). • Stimulation of the endometrium by estrogen (follicular and proliferative phase) followed by progesterone (luteal and secretory phase)= increases endometrial stores of arachidonic acid. • AA is a precursor to prostaglandin (PGF2),(PGE2) and leukotrienes. • Cyclooxygenase inhibitors decrease menstrual fluid prostaglandin levels and decrease pain.
CLINICAL MANIFESTATIONS • Occurs during ovulatory cycles. • The pain begins just before or with the onset of menstrual bleeding. • Gradually diminishes over 12 to 72 hours. • The cramps are confined to the lower abdomen (suprapubic). • Pain is strongest in the midline (back and thigh pain). • Nausea, diarrhea, fatigue, headache, and a general sense of malaise accompany the pain. • By comparison, women with secondary dysmenorrhea often have symptoms and physical findings that alert the physician to the presence of pelvic pathology (Endometriosis).
Treatment Nonpharmacological interventions • Heat • Dietary, vitamin, and herbal treatments • Exercise
Pharmacologic interventions: • A placebo • Nonsteroidal antiinflammatory agents (NSAIDs) • Hormonal contraceptives. • Levonorgestrel intrauterine contraception IUD
VAGINITIS • NORMAL VAGINAL PHYSIOLOGY AND FLORA : • Normal vaginal discharge consists of 1 to 4 mL fluid (per 24 hours). • White or transparent, thick, and mostly odorless. • Is formed by mucoid endocervical secretions in combination with sloughing epithelial cells, normal bacteria, and vaginal transudate. • The discharge may become more noticeable ( during pregnancy, use of estrogen-progestin contraceptives, midmenstrual cycle close to the time of ovulation. • The pH of the normal vaginal secretions is 4.0 to 4.5. • Dozens of different bacterial isolates. Lactobacillus Diphtheroids S. epidermidis
Infectious vaginitis : Common causes Bacterial vaginosis (40 to 50 percent of cases) Vulvovaginal candidiasis (20 to 25 percent of cases) Trichomoniasis (15 to 20 percent of cases) Less common causes Foreign body with secondary infection Desquamative inflammatory vaginitis Streptococcal vaginitis (group A) Ulcerative vaginitis associated with Staphylococcus aureus and toxic shock syndrome Idiopathic vulvovaginal ulceration associated with HIV. Noninfectious vaginitis : Chemical or other irritant Allergic, hypersensitivity, and contact dermatitis (lichen simplex) Traumatic vaginitis Atrophic vaginitis Postpuerperal atrophic vaginitis Desquamative inflammatory vaginitis (steroid-responsive) Erosive lichen planus Collagen vascular disease, Behcet's syndrome, Idiopathic vaginitis Causes of vaginitis
GENERAL DIAGNOSTIC APPROACH • History : Symptoms of vaginitis include abnormal vaginal discharge, pruritus, irritation, burning, soreness, odor, and, less commonly, dyspareunia • Physical examination : Appearance, cervical motion tenderness. The vulva usually appears normal in bacterial vaginosis. Erythema, edema, or fissure formation suggest candidiasis, trichomoniasis, or dermatitis.
Diagnostic studies Vaginal pH: • Vaginal pH is the single most important finding. • A strip of pH paper is applied to the vaginal sidewall. • A pH above 4.5 ina premenopausal woman suggests infections such as bacterial vaginosis or trichomoniasis (pH 5 to 6), and helps to exclude candida vulvovaginitis (pH 4 to 4.5). • Vaginal pH may be altered (usually to a higher pH) by contamination with lubricating gels, semen, douches, and intravaginal medications. Microscopy: • Candidal buds or hyphae • Motile Trichomonas • Epithelial cells studded with adherent coccobacilli (clue cells) • Polymorphonuclear cells (PMNs). • The saline should be at room temperature and microscopy should be performed within 10 to 20 minutes.
Vaginal discharge processing: • is generally sampled with a cotton-tipped swab. The sample of vaginal discharge is mixed with one to two drops of 0.9 percent normal saline solution on a glass slide. Cover slips are placed on the slides, which are examined under a microscope at low and high power. • The addition of 10 percent potassium hydroxide (KOH) to the wet mount of vaginal discharge destroys cellular elements (Candida vaginitis). • Smelling ("whiffing") the slide immediately after applying KOH is useful for detecting the fishy (amine) odor of Bacterial Vaginosis. • Excess WBCs without evidence of yeast, trichomonads, or clue cells suggests cervicitis. • If microscopy is not available, diagnostic testing cards are an alternative rapid test for confirming the clinical suspicion.
Vaginal culture: • For Candida or Trichomonas , if microscopy is negative because microscopy is not sufficiently sensitive to exclude these diagnoses in symptomatic patients. Cervical culture: • For cervicitis, typically due to Neisseria gonorrhoeae or Chlamydia trachomatis, if you see a purulent vaginal discharge, fever, or lower abdominal pain (PID). • Sexual behaviors that result in STD-related vulvovaginitis (eg, trichomoniasis, herpes simplex virus) increase the odds of acquiring other STDs. The presence of high risk behavior or any sexually transmitted disease requires screening for HIV, hepatitis B, and other STDs.
Clue Cell (BV)Bacteroides species; anaerobic Peptostreptococcus species; Fusobacterium sp. and Atopobium vaginae
Treatment Candida: A-non complicated • Butoconazole (Femstat)* • (Femstat)* 2 percent cream 5 g/day for 3 days or 1 day for sustained release formulation • (Gynazole) 2 percent cream 5 g/day for a single dose • Clotrimazole (Gyne- lotrimin, Mycelex)* 1 percent cream 5 g/day for 7 to 14 days • 100 mg vaginal tablet 1/day for 7 days • Miconazole (Monistat) 2 percent cream 5 g/day for 7 days • 100 mg vaginal suppository 1/day for 7 days • 200 mg vaginal suppository 1/day for 3 days • 1200 mg vaginal suppository 1 suppository • Tioconazole (Vagistat) 6.5 percent cream 5 g in a single dose • Terconazole (Terazol) 0.4 percent cream 5 g/day for 7 days • 80 mg vaginal suppository 1/day for 3 days • Nystatin (Mycostatin) 100,000 U vaginal tablet 1/day for 14 days • Fluconazole (Diflucan) B- complicated • Boric Acid
Trichomonas / BV Metronidazole • PO 500 mg bid x 7 days OR 2 gms single dose. • PV • Clindamycin 300 mg po bid x 5 days for BV. • Treat the partner in Trichomoniasis
Atrophic vaginitis • Lubricating /moisturizing gel. • Low dose Estrogen : • Systemic • Local