Download
1 / 82
830 likes | 1.21k Views
Chapter 14 – A Synopsis of the Cranial Nerves of the Brainstem. Michelle-Lee Jones February 18, 2009. OUTLINE. Introductory Points Cell Columns & Nuclei – Motor & Sensory Cranial Nerves of the Medulla Oblongata Cranial Nerves of the Pons-Medulla Junction Cranial Nerves of the Pons

E N D
Chapter 14 – A Synopsis of the Cranial Nerves of the Brainstem Michelle-Lee Jones February 18, 2009
OUTLINE • Introductory Points • Cell Columns & Nuclei – Motor & Sensory • Cranial Nerves of the Medulla Oblongata • Cranial Nerves of the Pons-Medulla Junction • Cranial Nerves of the Pons • Cranial Nerves of the Midbrain
Introductory Points • Regarding the brainstem: • Transit point for all ascending & descending tracts connecting the spinal cord to the forebrain • Associated with the exit/entry & nuclei of 10/12 cranial nerves • Lesions often involve cranial nerves & have long tract signs great localizing signs
Motor Cell Columns and Nuclei • Recap: basal plate derivatives CN motor nuclei oriented in discontinuous rostrocaudal cell columns • Nuclei from the same column possess common developmental, structural and functional features • 3 motor cell columns: • General Somatic Efferent (GSE), General Visceral Efferent (GVE) & Special Visceral Efferent (SVE)
Motor Cell Columns and Nuclei • GSE column features: • Most medial & anterior to the ventricular space • Nuclei include hypoglossal (XII), abducens (VI), trochlear (IV) & oculomotor (III) • Motor neurons innervate skeletal muscle from head mesoderm – tongue (occipital) & extraocular muscles (orbit) [ mesoderm NOT located in pharyngeal arches]
Motor Cell Columns and Nuclei 2. GVE – preganglionic parasympathetic column features: • Lateral to GSE • Forms cranial portion of craniosacral division of visceromotor system (parasympathetic) & preganglionic fibres travel on the CN • Nuclei include dorsal motor vagal nucleus (X), inferior salivatory nucleus (IX), superior salivatory nucleus (VII–intermediate), Edinger-Westphal nucleus (III) • Preganglionic axons peripheral ganglion postganglionic fibres visceral structure
Motor Cell Columns and Nuclei 3. SVE: • Most lateral motor column in medulla & pontine tegmentum • Nuclei include nucleus ambiguus (efferents on IX & X), facial motor nucleus & trigeminal motor nucleus • Muscles innervated originate from mesenchyme located within the pharyngeal arches
GSE GVE SVE
Sensory Cell Columns & Nuclei • Recap: alar plate derivatives CN sensory nuclei oriented in continuous cell column • Lateral location for sensory columns • 3 sensory cell columns: • Solitary tract and nucleus • Vestibular/cochlear nuclei • Trigeminal sensory nuclei
Sensory Cell Columns & Nuclei • Solitary tract & nucleus (CN VII, IX & X) • Visceral afferent centre of brainstem (solitary tract receives all the 1°visceral afferent central processes) • Taste or Special Visceral Afferent (SVA) fibres Gustatory nucleus (rostral area of solitary nucleus) • General Visceral Afferent (GVA) fibres Cardiorespiratory nucleus (caudal area of the solitary nucleus) • Solitary tract & nucleus (medulla) do not extend rostrally beyond the pons-medulla junction (most rostral CN = VII)
Sensory Cell Columns & Nuclei • Vestibular/cochlear nuclei • Just posterior to solitary tract & nucleus • Includes medial & spinal vestibular nuclei, anterior and posterior cochlear nuclei at pons-medulla junction, superior and lateral vestibular nuclei (caudal pons) • Sensory input from VIII only • Hearing (SSA, exteroceptive) & balance and equilibrium (SSA, proprioceptive)
Sensory Cell Columns & Nuclei • Trigeminal sensory nuclei • From spinal cord-medulla junction to rostral midbrain • 3 subdivisions • Spinal trigeminal nucleus (pars caudalis, pars interpolaris & pars oralis) – lateral medulla to caudal pons • Principal sensory nucleus (mid-pontine level) • Mesencephalic nucleus (lateral to periaqueductal grey)
Sensory Cell Columns & Nuclei • Trigeminal sensory nuclei • Principal sensory nucleus & particularly the spinal trigeminal nucleus GSA reception centre of brainstem • Receives all the general somatic afferent (pain & thermal) central processes • CN V, VII, IX & X
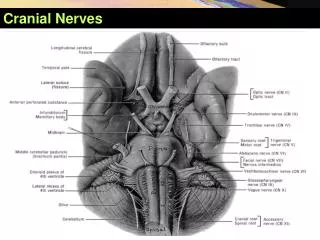
Cranial Nerves of the Medulla Oblongata (CN XII, XI, X & IX)
Hypoglossal Nerve (Motor) • Nucleus - internal to the hypoglossal trigone • Course: anterior medulla lateral aspects of medial lemniscus & pyramids pre-olivary fissure (rootlets) hypoglossal canal intrinsic tongue muscles + hypo-, stylo- & genioglossus muscles • Hypoglossal Canal: XII nerve, emissary vein, meningeal branch from ascending pharyngeal artery (dura posterior fossa)
Hypoglossal nucleus + fibres: • supplied by anterior spinal artery (ASA) • Medial Medullary Syndrome (ASA) • Deviation of tongue to side of lesion (GG) • Contralateral hemiparesis (CST) • Contralateral loss of position sense, vibration & 2-point discrimination (ML) • Root lesion – tongue deviation to side of lesion
Hypoglossal nucleus + fibres: • Internal capsule lesion • tongue deviation to the contralateral side (injury to crossed corticobulbar fibres innervating XII nucleus) • Contralateral hemiplegia • Drooping of facial muscles contralateral lower quadrant
Accessory Nerve (Motor): • SCM and trapezius muscles are innervated by motor neurons in the cervical spinal cord (NOT MEDULLA) • Cranial part of XI misnomer (XI fibres temporarily join vague, then separate to exit skull) • Course: Cervical SC axons exit SC laterally merge to form nerve foramen magnum briefly join caudal part of X in post. fossa jugular foramen
Accessory Nerve (Motor): • Root lesions: trapezius & SCM paralysis (ipsilateral shoulder droop & difficulty turning head to contralateral side) • C-spine lesion – above deficits are eclipsed by hemiplegia (CST) • Internal capsule lesion – similar deficits as above (uncrossed corticobulbar fibres to XI nucleus injured)
Vagus Nerve (Motor & Sensory): • Intermediate location (b/w midline & lateral medulla); exits post-olivary sulcus (exits cranial cavity via jugular foramen) • 2 ganglia immediately external to the foramen: • Superior Ganglion (GSA) • Inferior Ganglion (GVA, SVA)
Vagus Nerve - Motor cells of the medulla: 1. Dorsal motor nucleus of the vagus (GVE-PNS preganglionic) terminal (intramural) ganglia viscera (trachea, bronchi, heart, GI tract – just proximal to splenic flexure • Effects: bronchiole constriction, HR, blood flow, peristalsis, gut secretions 2. Nucleus Ambiguus (SVE) 4th pharyngeal arch muscles (refer to previous table)
Vagus Nerve – Sensory (GSA, GVA & SVA) • GSA (pain & thermal): • Small area of ear, part of external auditory meatus & dura posterior fossa superior ganglion (central processes to spinal trigeminal tract, thence to spinal trigeminal nucleus) • GVA & SVA: • Heart, aortic arch, pharynx & larynx, lungs, gut to level of splenic flexure (GVA) + taste buds on epiglottis & tongue base (SVA) inferior ganglion (central processes to solitary tract, thence to solitary nucleus - cardiorespiratory & gustatory portions
GSA SVA SVE GVE GVA
Vagus Nerve – Sensory (GSA, GVA & SVA) • Root lesion (vagus): dyphagia & dysarthria, no apparent lasting visceromotor dysfunction, taste NA & external auditory meatus GSA loss not key • Unilateral medulla injury nucleus ambiguus (Tumours, vascular lesions, syringobulbia) • Deficits as noted above • Bilateral medulla lesions aphonia, aphagia, dyspnea, or inspiratory stridor • Critical, especially if dorsal motor nucleus • Thyroid surgery recurrent laryngeal n. injury dysarthria
Glossopharyngeal Nerve (Motor & Sensory) • Leaves medulla @ postolivary sulcus, just rostral to vagus, leaves skull via jugular foramen • As with vagus, 2 ganglia: inferior ganglion (GVA, SVA) & superior ganglion (GSA)
Glossopharyngeal Nerve - Motor • Inferior salivatory nucleus (GVE PNS): axons join with tympanic nerve, then lesser petrosal nerve otic ganglion parotid gland • Nucleus ambiguus (SVE): innervation of stylopharyngeus that muscle that helps with swallowing & efferent part of gag reflex
Glossopharyngeal Nerve - Sensory • GSA: Pinna, external auditory canal superior ganglion • GVA: Parotid gland, oropharynx & carotid body inferior ganglion • SVA: Taste from posterior 1/3 inferior ganglion
Glossopharyngeal Nerve - Lesions • Rare, usually with X & XI roots @ jugular foramen • Nerve lesion: taste posterior 1/3, loss of ipsi. gag reflex (s-m X) • Glossopharyngeal neuralgia: • attacks of intense idiopathic pain in pharynx, caudal tongue, tonsil,? middle ear • Precipitated by spontaneous or artificial stimulation posterior oral cavity, swallowing or talking
SVA GSA GVE GVA SVE
Jugular Foramen & associated syndromes Right Jugular Foramen – medial, middle & caudal parts
Jugular Foramen & associated syndromes • Vernet syndrome • @ or just internal to the foramen • Loss of sensation post 1/3 tongue (IX); loss of sensation in larynx & pharynx, dysarthria & dysphagia (X); weakness of ipsil. SCM & trapezius (XI) • Collet-Sicard syndrome • Immediately external to the jugular foramen • Damage to IX, X, & XI + ipsil tongue weakness (hypoglossal canal is near foramen) • Villaret syndrome includes above + sympathetic fibres (SCG) ipsil Horner’s
Cranial Nerves of the Pons-Medulla Junction (CN VIII, VII & VI)
Vestibulocochlear Nerve (Almost exclusively sensory) • Most lateral, centrally related to cochlear & vestibular nuclei; 2 parts originate from specialized receptors within petrous temporal bone combined root in brainstem • Internal acoustic meatus (IAM) contains VIII, VII & labyrinthine artery • Cochlear part: • Cochlear Spiral ganglion (bipolar cells) IAM Cochlear nuclei (ant. & post.) brainstem relay nuclei MGN auditory cortex
Vestibulocochlear Nerve (Almost exclusively sensory) • Note cholinergic cells near the olivary nuclei olivocochlear tract (efferent cochlear bundle) inner & outer hair cells (dampen responses) • Vestibular part: • Ampullae of semicircular canals, utricle & saccule vestibular ganglion (bipolar cells) IAM PMJ vestibular nuclei (sup, inf, lat, med) in medulla & caudal pons cerebellum + oculomotor nuclei, etc.
Vestibulocochlear Nerve • VIII nerve lesions: hearing loss, tinnitus, vertigo, dizziness, ataxia • Cochlea, spiral ganglion or cochlear fibres lesions: ipsilateral sensorineural hearing loss • Lesions to brainstem or higher: ability to localise/interpret sound in space, no hearing loss per se • Conductive hearing loss: conduction through middle ear (typically ossicles) • Tinnitus pertains to auditory portion of VIII (peripheral or central damage)
Vestibulocochlear Nerve • Injury to vestibular fibres: vertigo (subjective – pt moves or objective – environment moves), nystagmus ± n/v • Nystagmus – vestibular influence over brainstem oculomotor control disconnected • Lesions of vestibular nuclei & central connections – vertigo, ataxia, nystagmus, ± n/v • Causes of vestibular dysfunction are myriad: • Meds, trauma, DM, cerebellar lesions, vestibular schwannoma etc. • Meniere’s syndrome: • hearing loss, sound distortion, vertigo, unsteadiness standing or walking • endolymphatic pressure size of utricle, saccule & cochlear
Facial Nerve (Motor & Sensory) (Petrous temporal bone) Sortie Intermediate nerve: GVE + SVA + GSA + few GVA
Facial Nerve • At geniculate ganglion (internal genu), greater petrosal nerve formed by GVE-preganglionic PNS nerves from VII joins deep petrosal nerve to form nerve of the pterygoid canal pterygopalatine ganglion • Post-ganglionic parasympathetic fibres join V2 orbit lacrimal gland • Small SVE branch stapedius muscle • Larger SVE branch (chorda tympani) middle ear joins V3 lingual branch preglanglionic PNS fibres to submandibular ganglion, collects SVA taste afferent fibres (ant 2/3 tongue) • SVE muscles of facial expression, post. belly digastric & stylohyoid
Facial Nerve • Sensory: • SVA: anterior 2/3 tongue lingual V3 changeover to chorda tympani to join VII nerve geniculate ganglion • GSA: fewer in number; external ear & external auditory canal central course on VII geniculate ganglion • GVA: few; mucous membrane of palate & nasopharynx geniculate ganglion enter brainstem in intermediate nerve