Met Hemoglobin
Practical Hematology Lab. - LAB 11 -. Met Hemoglobin. introduction.

Met Hemoglobin
E N D
Presentation Transcript
Practical Hematology Lab - LAB 11 - Met Hemoglobin
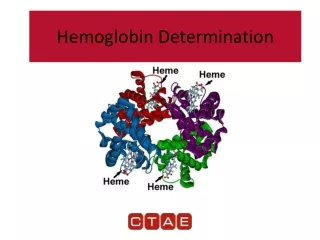
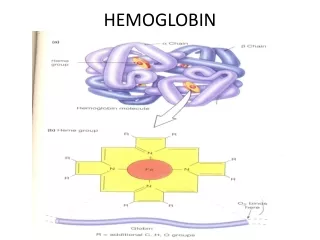
introduction • Methemoglobin (Hi) is a form of hemoglobin In which the ferrous ion( Fe2+) has been oxidized to the ferric state(Fe3+) and is, therefore, incapable of reversibly combining with oxygen (and, therefore, cannot transport the oxygen molecule). • Normally, a small amount of methemoglobin is continuously being formed in the red cell, but is, in turn, reduced by the red blood cell enzyme systems: • NADH methemoglobin reductase (cytochrome-b5 reductase) (major pathway). • NADPH methemoglobin reductase (minor pathway) • And to a lesser extent the ascorbic acid and glutathione enzyme systems.
Clinical significance • Increased amounts may be found in both hereditary and acquired disorders. • The hereditary form of methemoglobinemia is found in disorders in which the red blood cell reducing systems are abnormal and unable to reduce methemoglobin back to oxyhemoglobin. • In the presence of hemoglobin M, where the structure of the polypeptide chains making up the hemoglobin molecule is abnormal (there is a tendency toward oxidation of hemoglobin, with a decreased ability to reduce it back to oxyhemoglobin).
Clinical Significance • The acquired causes of methemoglobinemia are mainly due to certain drugs and chemicals, such as nitrates, nitrites, quinones, chlorates, sulfonamides and aniline dyes. • Normal Ranges • Methemoglobin is normally present in the blood in a concentration of 0.03 to 0.13 g/ dL, but a normal range should be determined by each laboratory. Slightly higher levels are present in infants and heavy smokers.
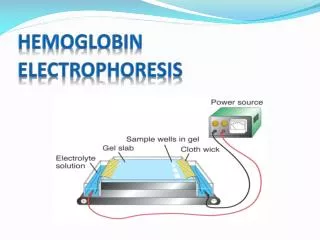
Principle • Whole blood is diluted with a phosphate buffer solution. • Methemoglobin has a maximum absorbance at a wavelength of 630 nm. • The diluted specimen is read in a spectrophotometer at 630 nm and the absorbance reading noted (D1). • Neutralized sodium cyanide is added to the mixture, converting the methemoglobin to cyanmethemoglobin, and read on the spectrophotometer (D2). • The change in optical density is directly proportional to the amount of methemoglobin present. • The methemoglobin in g/dL is then calculated using a factor, previously determined, for the spectrophotometer used.
Procedure Determination of calculation factor, F: • Before the methemoglobin results can be calculated, a calibration factor for the spectrophotometer being used must be determined. This is done one time only, or whenever a different spectrophotometer is used for the procedure. • Obtain a whole blood sample and determine the hemoglobin concentration in g/dL. • Place 5.0 mL of 0.017 M phosphate buffer into each of two test tubes. Add 50 µL of the whole blood specimen to one tube and mix. The second tube is to be used as the blank. • Add 20 µL of freshly prepared 20% potassium ferricyanide to both tubes. Mix and allow to stand for 2 minutes.
Procedure • Read on the spectrophotometer at 630 nm, using the blank to set the optical density at 0, and record the absorbance ( Dx). • Add 20 µL of neutralized sodium cyanide to both tubes. Mix and allow to stand for 2 minutes. Read on the spectrophotometer as above and record the optical density ( Dy). • F =Hgb (g/dL)/Dx - Dy
Procedure Procedure for testing patient specimen • Label and place 5 mL of 0.0 17M phosphate buffer into one tube for each specimen and control to be tested and one additional tube to serve as a blank. • Add 50 µL of whole blood to the appropriately labeled tube and mix well. Allow to sit at room temperature for 5 minutes . • Read on the spectrophotometer at a wavelength of 630 nm, using the blank to set the optical density at 0. Record the absorbance of the solution (D1) • Add 20 µL of neutralized sodium cyanide reagent to each tube including the blank, and mix. Allow to sit for 2 minutes. Read as in step c above record the optical density (D2).
Calculation of results Met hemoglobin (g/dL) = ( D1 – D2) x F Normal value Met hemoglobin <2% of total hemoglobin in normal blood, slightly higher in infants, particularly if premature. Note The presence of a large amount of SHb will result in an erroneously low measurement of total Hb.