Download
1 / 17
190 likes | 299 Views
Explore the intricate process of facial primordia, palate formation, and skull development from the expert perspective of Pamela Knapp, Ph.D., Professor of Anatomy & Neurobiology. Understand the crucial stages like merging vs. fusion, adult derivatives of facial prominences, and the formation of nasal cavities. Gain insights into clefting, palate development, and the intricate growth of facial structures in this detailed study.

E N D
Development of Face, Palate and Skull Pamela Knapp, Ph.D. Professor, Dept. Anatomy & Neurobiology MSB1 - Rm. 411 6-7570 peknapp@vcu.edu
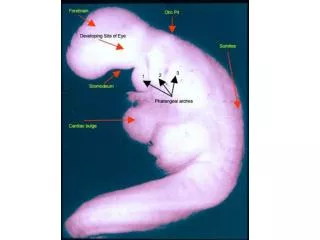
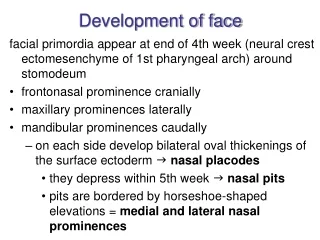
Facial primordia appear in the 4th week as a series of 5 ventral swellings NOTE: PA1 develops 2 prominences Frontonasal prominence - a single swelling located anterior to the stomodeum. NOT derived from pharyngeal arch tissue, but from mesenchyme proliferating ventral to the developing brain vesicles. Maxillary prominences - are paired swellings that are part of the pharyngeal arches. They lie lateral to the stomodeum and below the frontonasal prominence. Mandibular prominences - paired swellings that are posterior components of the 1st pharyngeal arch. They are found at the posterior border of the stomodeum Frontonasal prominence develops two lateral, ectodermal swellings, the nasal placodes. They will invaginate to form at first a nasal sac, and later a deeper nasal pit.
Merging vs. Fusion Merging - requires a continuous mesenchyme lying between ecto- and endoderm. Because of the presence of a continuous mesenchyme between the facial prominences, MERGING DRIVES FACIAL DEVELOPMENT! Incomplete merging? dimples …. clefts …. complete clefts Fusion -two separate tissue masses brought together Incomplete fusion also results in clefting
ln mn mx md md ---fnp--- Development of the mandibular prominences • L & R mandibular prominences are initially separated by • a groove. • Migration and proliferation of neural crest cells within the • pharyngeal arch causes merging of the prominences • and obliterates that groove. • Adult derivatives of the mandibular prominences include: • a) lower lip; b) chin; c) outer cheek
ln mn mx md md ---fnp--- Development of the frontonasal prominence FP gives rise to: forehead, the dorsum and apex of the nose, and several other structures important in face and palate development Nasal placodes are small lateral swellings that develop a deep nasal pit, with lateral and medial nasal prominences on each side. 2 medial nasal prominences expand and merge to form the intermaxillary segment. This segment will merge with maxillary prominences on either side Adult derivatives of the intermaxillary segment are: philtrum of the lip; primary palate. The last is an internal structure Incomplete merging between the intermaxillary segment and the maxillary prominences will cause cleft lip. Lateral nasal prominences also merge with the maxillary prominences, forming the alae (wings) of nose.
ln mn mx md md ---fnp--- Development of the maxillary prominences Maxillary prominences merge with the lateral nasal prominences and with the intermaxillary sement (the merged medial nasal prominences). A nasolacrimal groove originally separates the maxillary prominence from each lateral nasal prominence. A thick cord of tissue develops in this groove, and migrates down into underlying tissues. The cord is canalized, forming the open nasolacrimal duct. Adult derivatives of the maxillary prominences include: upper lip; inner cheek.
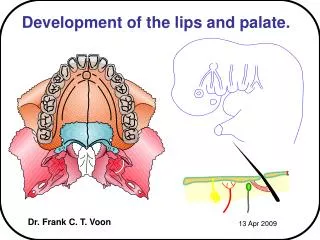
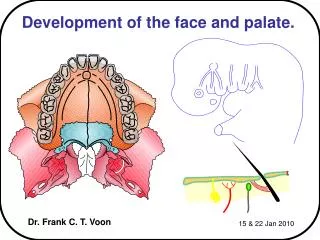
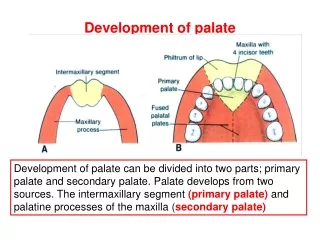
Palate Development All parts of the adult hard and soft palate are formed by medial growth of facial prominences. Recognize that facial prominences are 3-dimensional, and extend back into the developing head The primary palate (medial palatine process) forms from expansion of deeper portions of the intermaxillary segment. Primary palate forms only a small portion of the adult hard palate. Eventually ossifies and holds the incisor teeth. Secondary palate is forerunner of the rest of the adult hard AND soft palate. Forms from 6th-10th week. Until it has fully formed, the fetus has a common oronasal cavity.
Development of nasal cavities and secondary palate Nasal cavity is first indicated by a small nasal pit in center of nasal placode. Invaginates to larger nasal sac. Up to 6 weeks, a thin oronasal membrane separates the developing oral cavity (area of the pharynx just behind the stomodeum) and nasal cavity (the invaginating nasal sac). Nasal cavity enlarges and oronasal membrane ruptures, creating a single oronasal cavity, the primitive choana (behind the developing primary palate). Olfactory epithelium by 7th week. Secondary palate fully formed and joined with primary palate by 12 weeks. This separates oral and nasal cavities at forward ends. A definitive choana lies behind the secondary palate. NOT SEEN IN THIS SECTION: The nasal septum is forming - it will grown down at midline to meet the secondary palate. This will create right and left nasal cavities, each of which opens into the pharynx behind the secondary palate (at definitive choana).
The secondary palate is formed from 2 lateral palatine processes (palatine/palatal shelves) that extend medially from the lateral surface of the maxillary prominence. Same tissue forms the inner cheek and upper lip on the external surface. At first, the LPPs grow downward, along the side of the tongue (developing on the floor of the pharynx). Note the nasal septum, growing downward at midline from tissue of the frontonasal prominence. LPPs slip above the tongue, and begin to grow towards each other. They normally meet and fuse rapidly. When the LPPs have also fused with the nasal septum AND the primary palate, then the full palate has been created, along with separate right and left nasal cavities.
The incisive foramen is the site of fusion of the primary and secondary palates. Fusion of the LPPs occurs anterior to posterior. Ossification occurs throughout the primary and secondary palate, except for the portion that lies posterior to points of fusion with the nasal septum … including the uvula. The ossified portions are the hard palate. The unossified portions (including uvula) are the soft palate. The site of fusion of the LPPs is termed the palatal/palatine raphe.
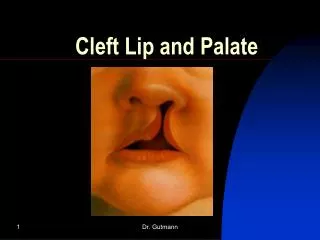
Anomalies of face and palate development Clefts are breaks between two tissue areas - failure to merge or fuse completely. Underlying explanation is problem with mesenchyme migration or proliferation (frequently a neural crest issue). Etiology of clefting - multifactorial -genetic -environmental factors during critical period (7-12 weeks). Include exposure to alcohol, Vitamin A derivatives, steroids. Cleft lip is overall more common than cleft palate (1 in 1000 vs. 1 in 2,500 live births) Cleft palate is more common in female infants. Anterior clefts - involve tissue anterior to incisive foramen (lip +/- palate) Posterior clefts - involve tissue posterior to incisive foramen (palate only) Looks like Unilateral anterior cleft - a.k.a. left side cleft lip. ((Cannot see from this view if either palate is involved.)) Bilateral anterior cleft with palate involvement. ((Cannot see if cleft extends to secondary palate) Looks like unilateral anterior cleft lip and palate with secondary palatal cleft.
How do these things happen? Anterior Clefts: Failure of merging between intermaxillary segment and maxillary prominence explains both lip and palate cleft. “A and B” above show unilateral complete & bilateral complete anterior cleft. Partial anterior cleft is lip only. (Disagreement over merging vs. fusion IMS with secondary palate). Posterior Clefts: Failure of fusion of the two lateral palatine processes. Complete posterior cleft: Affects secondary palate along entire length. Includes hard and soft portions. Shown in “C”. Partial posterior cleft: Can affect any portion of the secondary palate (ex: cleft uvula). Combinations of anterior and posterior clefts are possible. “D” shows combined complete bilateral anterior and posterior clefting.
Max Mand If the maxillary processes and lateral nasal processes do not merge, an oblique facial cleft is created. The nasolacrimal ducts are exposed to the facial surface (persistant nasolacrimal grooves). Can be combined with a cleft lip (as in “A” above) if the intermaxillary segment also does not merge with the maxillary processes. Macrostomia (large mouth) occurs with failure of lateral merging of the maxillary and mandibular prominences. The mouth opening can extend to the ears. Microstomia (small mouth) results from excessive merging of the same. Can be unilateral or bilateral. When the medial nasal prominences do not completely merge in the region of the intermaxillary segment, a median cleft lip is formed (“C” above).
Prechordal cartilages Region of occipital somites Two parts of the adult skull: Neurocranium (encloses brain): composed of cartilaginous floor (chondrocranium) and membranous vault. Viscerocranium (encloses face) First part of the adult skull to form is the floor of the neurocranium - the cartilaginous chondrocranium. Forms as a cartilaginous structure, from multiple chondrification centers. Mesenchyme that forms the cartilage derives from occipital somites and from somitomeres. Multiple smaller cartilages that are generated then fuse. The cartilage is later replaced by bone - “endochondral ossification” Existance of separate chondrification centers is important!! They allow for formation of foramina - the passageways for blood vessels and nerves accessing the cranial vault. Skull Development Cartilages of the Median Cartilaginous Plate a. Occipital cartilage - Formed from sclerotome cells in several occipital somites. b. Parachordal cartilages - Formed by cells of somitomeres at tip of notochord. a+b most of occipital bone c. Prechordal cartilages - 2 pair c1. hypophyseal, forms around pituitary c2. trabecular Hypophyseals much of body of sphenoid bone (includes sella turcica) Trabecular some sphenoid & some ethmoid bone Formation of the cartilaginous plate
Endochondral ossification - replacement of chondrocranial cartilage models by bone, occurs in multiple centers of ossification which appear between the 8th and 16th wks • Additional chondrification centers form lateral cartilaginous structures that fuse with the median cartilaginous plate (blue color in diagrams). Nasal capsules - develop around the nasal sacs Otic capsules - form otic vesicles -these later fuse with the median cartilaginous plate.3. Alisphenoid cartilages - form greater wings of sphenoid bone4. Orbitosphenoid cartilages - form lesser winds of sphenoid boneNOTE: openings for nerves and blood vessels formed as median and lateral component cartilages fuse.
Formation of the membranous neurocranium (cranial vault) Membranous neurocranium (cranial vault) is made of the large, flat bones of the skull -parietal, frontal, squamous part of temporal, interparietal part of occipital, outer part of greater wing of sphenoid. These form by intramembranous ossification (mesenchyme transforms directly into bone) -different than bones in the chondrocranium (floor), which went through a cartilage step. -each develop from separate ossification centers. During fetal life and in infancy, the flat bones forming the cranial vault are separated by fibrous connective tissue sutures. Fontanelles are fibrous areas at the intersection of the sutures. -largely close by end of 1st year, except for anterior fontanelle. Utility of fontanelles and sutures is that they allow for a change in skull shape during the birth process. -also used clinicall for assessing hydration, intracranial P, and assessing growth parameters by comparing to normal ossification schedule.
Development of viscerocranium There are components that form from mesenchyme both directly (ie, by intramembranous ossification) and with an intermediate cartilage step (by endochondral ossification). Membranous Viscerocranium Multiple centers of ossification exist within the prominences of the 1st pharyngeal arch (mandibular and maxillary) Bones: nasal, premaxilla, maxilla, lacrimal, vomer, zygomatic, palatine, sphenoid (part of greater wing), temporal (squamous and tympanic) Cartilaginous Viscerocranium Derived from cartilages of the pharyngeal arches (see chart PA lecture) Parts of PA arch cartilages I-IV and VI persist. Bones: incus, malleus, stapes, styloid process, hyoid bone, mandible Cartilages of arch IV and VI remain unossified, and form cartilages of the larynx and trachea.