Download
1 / 23
260 likes | 794 Views
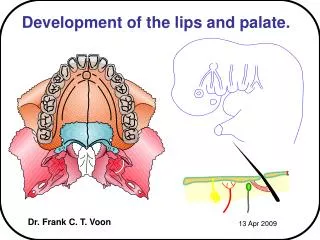
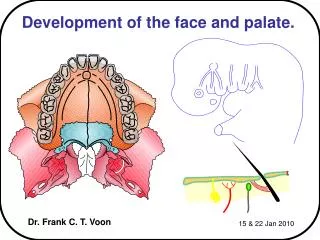
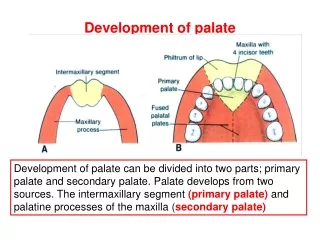
Development of palate. Development of palate can be divided into two parts; primary palate and secondary palate. Palate develops from two sources. The intermaxillary segment (primary palate) and palatine processes of the maxilla ( secondary palate).

E N D
Development of palate Development of palate can be divided into two parts; primary palate and secondary palate. Palate develops from two sources. The intermaxillary segment (primary palate) and palatine processes of the maxilla (secondary palate)
Intermaxillary segment is formed by the fusion of the two medial nasal prominences (globular prominences)
Development of palate Intermaxillary segment has three components superficial part (Labial) – philturm of upper lip, Middle part(Jaw) – part of maxilla bearing incisor teeth Deep part(Palatal components) – palate infront of the incisive fossa (primary palate)
Development of palate Primary palate develops from the intermaxillary segment The main part of the definitive palate(secondary) is formed by two shelf like outgrowths from the inner surface of the maxillary prominences
Development of palate These are called palatine process, which appear in the 6th week as extensions of the maxillary prominences
Development of palate Palatine shelf – from maxillary prominence. Oblique in position, on either side of the tongue Palate after the removal of the lower jaw
Development of palate They are directed obliquely downwards on either side of the developing tongue
Development of palate In the seventh week these shelves become horizontal due to the downward movement of the developing tongue Finally the two palatine shelves meet in the midline and fuse forming the secondary plate
Development of palate Anteriorly the shelve fuse with the triangular primary palate The incisive foramen is the midline landmark between the primary and secondary palate
Development of palate Same time when the palatine shelves fuse with each other the nasal septum grows downwards and fuses with superior aspect of the palate
Development of palate Fusion of the palatine shelves and the nasal septum which is formed by the frontonasal prominence
Palate and its components Part infront of incisive fossa – intermaxillary segment (primary palate) Part behind incisive fossa- palatal process of maxilla (secondary palate) Anterior part becomes ossified to form hard palate, posterior part - soft palate Muscles develop from 4th arch mesoderm , except tensor palatine
Congenital anomalies • Cleft palate (Anterior) In this anomaly cleft is present between primary and secondary palate. The cleft extends from incisive fossa to upper jaw, lateral to lateral incisor. Due to the failure of the fusion between palatal process and primary palate. Posterior cleft palate -Here the cleft is restricted to posterior palate behind the incisive fossa. In this anomaly two palatal processes fail to fuse with each other.
Complete cleft palate In this anomaly the cleft is Y shaped .Here the palatal processes not only fail to fuse with each other but also fail to fuse with the primary palate. In all types of cleft palate there is communication between oral and nasal cavities. There is regurgitation of fluid into nasal cavity during swallowing. The cleft palate is a genetic anomaly but sometimes it can be because of teratogenic effect of some drugs during pregnancy.
Types of cleft lip and palate – anterior defects Incomplete cleft lip Bilateral cleft lip Cleft lip, cleft jaw, and cleft palate Anterior cleft varies in severity. Defect in vermilion of the lip This may extend to the nose More severe cases – cleft extends to the jaw splitting maxilla between lateral incisor and canine tooth Frequently such cleft extends to the incisive foramen
This due to lack of fusion between the palatine shelves (isolated cleft palate) Smallness of shelves Failure of the shelves to elevate Failure of the tongue to drop because of micrognathia Cleft palate is less frequent than cleft lip Occurs more often in females In females the palatal shelves fuse one week later than males which may explain why it is more common in females Drugs (anticonvulsant) like phenobarbital and dyphenylhydantoin given during pregnancy increase the risk Cleft palate- posteior defect Isolated cleft palate
Cleft palate Third category is formed by the combination of clefts lying anterior and posterior to incisive foramen There may be complete cleavage of the secondary palate, Cleavage of the uvula of varying degree Failure of fusion of secondary palate anteriorly with the primary plate Cleft palate combined with anterior cleft lip
Development of nasal cavity 6th week nasal pits deepen considerably due to the growth of surrounding nasal prominences and partly because of penetration into the underlying mesoderm.
Development of nasal cavity This is the primitive nasal cavity. It is separated from the oral cavity by oronasal (bucconasal) membrane. It is formed by the ectoderm of both nasal and oral cavities The floor of the cavity is formed by primitive palate
Development of nasal cavity Oronasal membrane breaks and results in the formation of a communication – the primitive posterior nasal aperture (choanae) Once the secondary palate develops the posterior nasal aperture shifts posteriorly to form definitive posterior nasal aperture
Paranasal air sinuses • Develop as diverticula of the lateral wall of the nasal cavity • They extend in to the maxilla, ethmoid, sphenoid and frontal bones • They reach their maximum size during puberty • They contribute to the definitive shape of the face