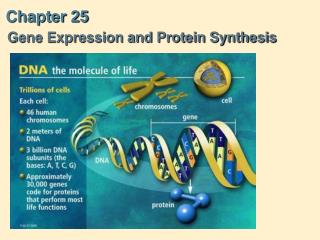
Overview of the Urinary System and Kidney Function
The urinary system plays a critical role in maintaining fluid homeostasis, regulating blood pH, and eliminating waste products from the body. The kidneys, crucial organs in this system, are responsible for filtering blood and forming urine through the processes of filtration, reabsorption, and secretion. They also perform essential endocrine functions, such as releasing hormones like erythropoietin and renin. Understanding the anatomy and physiology of nephrons, the functional units of the kidneys, is key to appreciating their roles in metabolism and waste management.

Overview of the Urinary System and Kidney Function
E N D
Presentation Transcript
Chapter 25 The Urinary System G.R. Pitts, J.R. Schiller, and James F. Thompson, Ph.D.
General • During metabolism cells produce wastes • waste - any substance acquired or produced in excess with no function in body • e.g. - CO2, H2O, heat • All wastes must be eliminated, or at least maintained at low concentrations • Additionally, protein breakdown leaves nitrogenous wastes • Excess sodium (Na+), chloride (Cl-), potassium (K+), sulfate (SO42-), phosphate (PO42-), and hydrogen ion (H+) must be regulated
General • Several organs transport, neutralize, store and remove wastes • Body fluid and body fluid buffers • Blood and blood buffers • Liver • Lungs • Sudoriferous (sweat) glands (minor) • Hair and nails (minor) • GI tract and liver • Kidneys
General • Urinary system • Maintains fluid homeostasis including: • regulation of volume and composition by eliminating certain wastes while conserving needed materials • regulation of blood pH • regulation of hydrostatic pressure of blood and, indirectly, of other body fluids • Contributions to metabolism • helps synthesize calcitriol (active form of Vitamin D) • secretes erythropoietin • performs gluconeogenesis during fasting or starvation • deaminates certain amino acids to eliminate ammonia
Kidneys • Paired reddish organs, just above waist on posterior wall of abdomen • partially protected by 11th, 12th ribs • right kidney sits lower than the left kidney • receive 20-25% of the resting cardiac output • Consume 20-25% of the O2 used by the body at rest
Kidneys (cont.) • Retroperitoneal, as are ureters and urinary bladder
Kidney - Internal Gross Anatomy Know these terms for lecture and lab exams!
Kidney - Internal Micro Anatomy • Nephron – the functional unit of kidney • Three physiological processes: 1) filtration, 2) reabsorption , and 3) secretion • These three processes cooperate to achieve the various functions of the kidney • Different sites different primary functions
The Functions of the Kidney • Nephron forms urine from blood plasma • 1) formation of a plasma filtrate • 2) reabsorption of useful molecules from the filtrate to prevent their loss in urine • 3) secretion of excess electrolytes and certain wastes (nitrogenous wastes, H+) in concentrations greater than their concentration in plasma • 4) regulation of water balance by concentrating or diluting the urine • 5) minor endocrine function – releasing hormone erythropoietin to stimulate RBC production • 6) releasing renin for angiotensinogen activation
Kidney - Internal Micro Anatomy • ~A million nephrons are located in the cortex • The filtrate is carried by the collecting duct system through the medulla • The urine is collected at the papillae into the minor and major calyxes Nephron Papilla Minor Calyx
Renal Corpuscle Renal Tubule Nephron • 2 major parts to the nephron
Nephron • Renal corpuscle • site of plasma filtration • 2 components • glomerulus • tuft of capillary loops • fed by afferent arteriole • drained by efferent arteriole • glomerular (Bowman's) capsule • double walled cup lined by simple squamous epithelium • outer wall (parietal layer) separated from inner wall (visceral layer = podocytes) by capsular (Bowman's) space • as blood flows through capillary tuft – filtration occurs • water and most dissolved molecules pass into capsular space • large proteins and formed elements in the blood do not cross
Nephron • Renal tubule - where filtered fluid passes from capsule • proximal convoluted tubule (PCT) • loop of Henle (nephron loop) • distal convoluted tubule (DCT) • short connecting tubules • collecting ducts • merge to papillary duct • then to minor calyx • 30 pap ducts/papillae DCT PCT ducts Loop
Nephron • Cortical vs. juxtamedullary nephrons • Location related to the length of loop of the nephron • 15-20% of the nephrons have longer loops and increased involvement inthe reabsorption of water H2O
Renal Corpuscle Histology • Each nephron portion has distinctive features • Histology of the glomerular filtration membrane • Three components to the filter • From inside to out, the layers prevent movement of progressively smaller particles
Histology of Filtration Membrane • Endothelium of glomerulus • Single layer of capillary endothelium with fenestrations • Prevents RBC passage; WBCs use diapedesis to get out
Histology of Filtration Membrane • Basement membrane of glomerulus • Between endothelium and visceral layer of glom. capsule • Prevents passage of large protein molecules
Histology of Filtration Membrane • Filtration slits in podocytes • Podocytes • specialized epithelium of visceral layer • footlike extensions with filtration slits between extensions • Restricts passage of medium-sized proteins
Tubule Histology • PCT - cuboidal cells with apical microvilli • Descending Loop, and beginning of Ascending Loop • simple squamous epithelium • water permeable • Remainder of Ascending limb of the Loop • cuboidal to low columnar epithelial cells • impermeable to water • permeable to solute (ions) • DCT, collecting ducts • cuboidal with specialized cells • principal cells - sensitive to ADH (antidiuretic hormone) • intercalated cells - secrete H+
Renal Blood Supply • Important vessels • Renal arteries • 20-25% of resting CO • 1200 ml/min • Segmental arteries • Interlobar arteries - through columns • Arcuate arteries • Interlobular arteries Refer to the kidney models in lab.
Renal Blood Supply peritubular capillaries • Important vessels • Afferent arterioles - each renal corpuscle receives one • Glomerular capillaries • Efferent arterioles - drain blood from glomerulus cortex -------- medulla • Peritubular capillaries - around cortical nephrons • Vasa recta - long networks from the efferent arteriole around the Loop (juxtamedullary nephrons) Vasa recta
Renal Blood Supply • Important vessels • Interlobular veins • Arcuate veins • Interlobar veins • Segmental veins • Renal veins - exits hilus Refer to the kidney models in lab.
Renin-Angiotensin System • Juxtaglomerular apparatus (JGA) • Distal tubule contacts afferent arteriole at renal corpuscle • Juxtaglomerular (JG) cells • modified smooth muscle cells in afferent arteriole wall detect changes in blood pressure (a stretch reflex) • Secrete enzyme renin to trigger Renin-Angiotensin System if blood pressure falls JG afferent art. efferent art. Distal Convoluted Tubule
Renin-Angiotensin System • Juxtaglomerular apparatus (JGA) • Distal tubule contacts afferent arteriole at renal corpuscle • Macula Densa (MD) cells • special cells in the wall of the distal tubule in this area monitor the osmotic potential in the filtrate in the distal tubule • stimulate JG cells to release renin if filtrate is too dilute, indicating insufficient filtration and/or low blood pressure/low blood volume • Both JG and MD cells work together to regulate blood pressure and blood volume JG afferent art. MD efferent art. Distal Convoluted Tubule
Renin-Angiotensin System • Hepatocytes secrete inactive precursor Angiotensinogen into the bloodstream • Juxtaglomerular (JG) cells secrete the enzyme reninto convert Angiotensinogen to Angiotensin I in the bloodstream • Angiotensin I is transported to the lungs where Angiotensin Converting Enzyme (ACE) converts Angiotensin I to Angiotensin II • Both Angiotensin I and Angiotensin II act as circulating hormones to increase blood pressure and blood volume; AII is stronger
Renal Nerve Supply • Nerves from renal plexus of Sympathetic Division of ANS innervate the kidney • Vasomotor nerves accompany the renal arteries and their branches • What is the role of sympathetic stimulation on renal blood flow? • In “Fight or Flight” or muscular exertion: • decrease renal arterial flow • decrease urine production • maintain blood volume • increase systemic blood pressure
Physiology of Urine Formation • Glomerular filtration - first step in urine formation • forcing of fluids and dissolved solutes through membrane by hydrostatic pressure • same process as in systemic capillaries • results in a filtrate • 180 L/day, about 60 times plasma volume • 178-179 L/day is reabsorbed (~99%) 1-2 L/day of urine is typical
Glomerular Filtration • 3 structural features of the renal corpuscles enhance their filtering capacity: • Glomerular capillaries are relatively long which increases theirsurface area for filtration • Filter (endothelium-capsular membrane) is thin and porous • Fenestrated glomerular capillaries are 50 times more permeable than regular capillaries • The filtration slits of the basement membrane only permit passage of small molecules • Glomerular Capillary blood pressure is high – the efferent arteriole diameter is less than the afferent arteriole diameter -- increasing filtration pressure in the renal corpuscle
Glomerular Filtration • Net filtration pressure (NFP) depends on 3 pressures: • glomerular blood hydrostatic pressure (GBHP) • capsular hydrostatic pressure (CHP) • blood colloid osmotic pressure (BCOP) NFP = GBHP – CHP – BCOP 10 = 55 - 15 - 30 1 2 3
Glomerular Filtration Rate (GFR) • GFR • Volume of filtrate that forms in all renal corpuscles in both kidneys/min • Adult’s GFR 125 mL/min (180 L/day) • Regulation of GFR • When more blood flows into glomerulus, GFR • GFR depends on systemic blood pressure, and the diameter of afferent & efferent arterioles • If glomerular capillary blood pressure falls much below 45 mm Hg, no filtration occurs anuria (no urine output)
Glomerular Filtration Rate (GFR) • 3 principal regulators of GFR: • Renal autoregulation of GFR • the kidneys are able to maintain a relatively constant internal blood pressure and GFR despite changes in systemic arterial pressure • there is negative feedback from the JuxtaGlomerular Apparatus adjusting blood pressure and blood volume
Glomerular Filtration Rate (GFR) • 3 principal regulators of GFR (cont.): • Hormonal regulation of GFR • Angiotensin I & II • activated by renin released from JG cells and further by ACE in the lungs • 5 important functions • direct vasoconstriction • aldosterone secretion • thirst generated at the hypothalamus • ADH secretion • Na+ reabsorption (H2O follows passively) • Net Effect increased blood pressure and blood volume
Glomerular Filtration Rate (GFR) • 3 principal regulators of GFR (cont.): • Hormonal regulation of GFR • Angiotensin I & II • Atrial Natriuretic Peptide (ANP) • secreted by cells in atria of heart in response to stretch • GFR, promotes excretion of H2O, Na+, but retention of K+ • suppresses output of ADH, aldosterone, and renin • Net Effect decreased blood pressure and blood volume • Aldosterone • secreted by cells in adrenal cortex in response to angiotensin I & II (and ACTH) • GFR, promotes retention of H2O, Na+, but excretion of K+ • antagonist to Atrial Natriuretic Peptide • Net Effect increased blood pressure and blood volume
Glomerular Filtration Rate (GFR) • 3 principal regulators of GFR (cont.): • Neural regulation • kidney’s blood vessels supplied by vasoconstrictor fibers from Sympathetic Division of ANS which release Norepinephrine • strong sympathetic stimulation causes JG cells to secrete renin and the adrenal medulla to secrete Epinephrine
GFR Control modest
Tubular Reabsorption • Movement of water and certain solutes back into bloodstream from the renal tubule • Filter 180 L/day of fluid and solutes • nutrients (Na+, K+, Glucose, etc.) are needed by body • body will expend ATP to get them back into blood • about 99% of the filtrate volume is reabsorbed from the tubule by active transport and osmosis • Epithelial cells in PCT (microvilli) increase surface area for tubular reabsorption • DCT and collecting ducts play a lesser role in nutrient/solute reabsorption
Reabsorption of Na+ in PCT • PCT is site of most electrolyte reabsorption • Mechanisms which aid Na+ transport • Na+/ K+ ATPase on basolateral side is fundamental • Concentration of Na+ inside the tubular cells is low • Interior of the cell negatively charged • Double gradient for Na+ movement from filtrate to tubular cell • Requires ATP energy
Reabsorption of Nutrients in PCT • ~100% of the filtered glucose and other sugars, AA's, lactic acid, and other useful metabolites are reabsorbed • Na+ symporters power secondary active transport systems • Why secondary? They rely on the Na+/ K+ ATPase pump.
Reabsorption of Na+ in PCT • Na+ is passively transported from the filtrate in tubule lumen into tubular cells to replace the Na+ being actively transported into the peritubular capillaries. Glucose moves with Na+.
Reabsorption of H2O in PCT • H2O follows Na+ passively by osmosis from the filtrate through the tubular cells into the peritubular capillaries
Reabsorption of Nutrients in PCT • The movement of water back to the bloodstream concentrates the remaining solutes in the filtrate [H2O] [solutes]
Reabsorption of Nutrients in PCT • The new concentration gradients increase the diffusion of some of the other remaining solutes in the filtrate from lumen to the blood stream.
Transport Maximums (Tm)’s • each type of symporter has an upper limit (maximum) on how fast it can work • any time a substance is in the filtrate in an amount greater than its transport maximum, some of it will be left behind in the urine • only Na+ has no transport maximum because Na+ is being actively transported by the Na+/ K+ ATPase pump at all times.
Renal Thresholds • The Renal Threshold is the plasma concentration at which a substance begins to spill into the urine because its Tm has been surpassed. • If the plasma filtrate concentration is too high, all of the substance cannot be reabsorbed. • For example, glucose spills into the urine in untreated diabetics. • Tm for glucose = 375 mg/min • If blood glucose > 400 mg/100 mL, large quantities of glucose will appear in the urine
Reabsorption in the PCT • By the end of the PCT the following reabsorption has occurred: • 100% of filtered nutrients (sugars, albumin, amino acids, vitamins, etc.) • 80-90% of filtered HCO3- • 65% of Na+ ions and water, • 50% of Cl- and K+ions
Reabsorption in Loop of Henle • Cells in the thin descending limb are only permeable to water • H2O reabsorption is not coupled to reabsorption of filtered solutes (osmosis) in this area as it had been in the PCT • [Note: illustration at right is not thin descending limb of nephron loop]
Reabsorption in Loop of Henle • Cells in the thicker ascending Loop feature sodium-potassium-chloride symporters • reabsorb 1 Na+, 1 K+, 2 Cl- • depend on the low cytoplasmic Na+ concentration to function • little or no H2O is reabsorbed from the thick ascending Loop • Loop reabsorbs 30% of K+, 20% of Na+, 35% of Cl-, and 15% of H2O • H2O reabsorption is not coupled to reabsorption of filtered solutes (osmosis)
Reabsorption in DCT and Collecting Ducts • Filtrate reaching the DCT has already had ~80% of the solutes and H2O reabsorbed • Fluid now has the characteristics of “urine” • DCT is the site of final adjustment of urine composition • less work to do, so no need for microvilli = brush border to increase surface area for tranporters • Na+/K+/Cl- symporter is a major DCT transporter • DCT reabsorbs another 10% of filtrate volume
Reabsorption in DCT and Collecting Duct • Principal cells are present in the distal DCTs and collecting ducts • 3 hormones act on principal cells to modify ion and fluid reabsorption • [1] Anti-Diuretic Hormone (ADH) (from neurohypophysis) • H2O reabsorption by increasing permeability to H2O in the DCT and collecting duct • details discussed later on