Download
1 / 79
810 likes | 1k Views
Chapter 19: Blood. The Cardiovascular System. A circulating transport system that consists of: a pump (the heart) a conducting system (blood vessels) a fluid medium (blood) Functions of the Cardiovascular System:. To transport materials to and from cells: - O2 & CO2

E N D
The Cardiovascular System • A circulating transport system that consists of: • a pump (the heart) • a conducting system (blood vessels) • a fluid medium (blood) Functions of the Cardiovascular System: • To transport materials to and from cells: • - O2 & CO2 • - nutrients • - hormones • - immune system components • - waste products
Fluids of the Body • Cells of the body are serviced by 2 fluids blood • composed of plasma and a variety of cells • transports nutrients and wastes interstitial fluid • bathes the cells of the body • Nutrients and oxygen diffuse from the blood → interstitial fluid → cells • Wastes move in the reverse direction • Hematology is study of blood and blood disorders
Blood • Fluid connective tissue • Functions include • Transporting dissolved gases, nutrients, hormones, and metabolic wastes • Regulating pH and ion composition of interstitial fluids • Restricting fluid loss at injury sites • Defending the body against toxins and pathogens • Regulating body temperature by absorbing and redistributing heat Physical Characteristics of Blood • Thicker (more viscous) than water and flows more slowly than water • Temperature of 100.4◦ F (38◦ C) • pH 7.4 (7.35-7.45) • 8 % of total body weight • Blood volume : 5 to 6L in average male ; 4 to 5L in average female • : hormonal negative feedback systems maintain constant • blood volume and osmotic pressure
Blood Plasma • 0ver 90% water • 7% plasma proteins -created in liver - confined to bloodstream • Albumin • maintain blood osmotic pressure • Globulins (immunoglobulins) • antibodies bind to foreignsubstances called antigens • form antigen-antibody complexes Transport globulins (small molecules): • hormone-binding proteins • Metalloproteins & apolipoproteins (lipoproteins) • steroid-binding proteins • Fibrinogen • Produce fibrinogen for clotting
Other Plasma Proteins • 1% of plasma: • changing quantities of specialized plasma proteins • enzymes, hormones, and prohormones Origins of Plasma Proteins : • 90% made in liver • Antibodies made by plasma cells • Peptide hormones made by endocrine organs Serum -liquid part of a blood sample in which dissolved fibrinogen has converted to solid fibrin ; it is plasma minus clotting proteins Other Substances • 2% of plasma • electrolytes, nutrients, gases, waste products
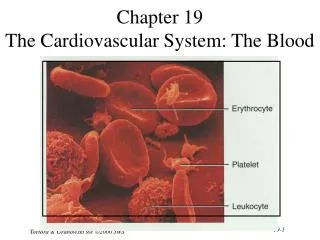
Formed Elements of Blood • Red blood cells ( erythrocytes ) – transport oxygen • White blood cells ( leukocytes ) – immune functions • granular leukocytes : neutrophils, eosinophils, basophils • agranular leukocytes • lymphocytes = T cells, B cells, and natural killer cells • Monocytes • Platelets (special cell fragments) – blood clotting • Only WBCs are complete cells • RBCs have no nuclei or organelles, and platelets are just cell fragments • Most formed elements survive in the bloodstream for only a few days • Most blood cells do not divide but are renewed by cells in bone marrow
Hematocrit • Percentage of blood occupied by cells • female normal range • 38 - 46% (average of 42%) • male normal range • 40 - 54% (average of 46%) • testosterone • Anemia • not enough RBCs or not enough hemoglobin • Polycythemia • too many RBCs (over 65%) • dehydration, tissue hypoxia, blood doping in athletes
Erythrocytes (RBCs) • Most numerous of the formed elements • Females: 4.3–5.2 million cells/cubic ml • Males: 5.2–5.8 million cells/cubic ml • Biconcave disc • Folding increases surface area (30% more) • Plasma membrane contains spectrin • Give erythrocytes their flexibility -7.8 µm RBC passes through 4 µm capillary • Anucleate, no centrioles, no organelles • End result - no cell division • No mitochondria means they generate ATP anaerobically • Prevents consumption of O2 being transported • Filled with hemoglobin (Hb) - 97% of cell contents • Hb functions in gas transport • Hb + O2 HbO2 (oxyhemoglobin)
Hemopoiesis: formation of blood cells • Also known as hematopoiesis • Occurs in the red marrow (found in spaces of spongy bone): • In adults, mostly in the proximal epiphysis of femur and bodies of the lumbar vertebrae • Originally from pluripotent stem cells from mesenchyme • In the fetus, hematopoiesis occurs in the liver, spleen, thymus, lymph nodes and yolk sac • Erythropoietin from the kidneys stimulates hematopoiesis
Erythrocyte development Myeloid Stem Cell Components needed for RBC: -amino acids -iron -vit. B12, B6, and folic acid - carbohydrates - lipids
Erythrocyte Function • Erythrocytes are dedicated to respiratory gas transport • Hemoglobin reversibly binds with oxygen and most oxygen in the blood is bound to hemoglobin • Composition of hemoglobin • A protein called globin • made up of two alpha and two beta chains • A heme molecule • Each heme group bears an atom of iron, which can bind to one oxygenmolecule • Each hemoglobin molecule thus can transport four molecules of oxygen (oxyhemoglobin) • Each RBC contains an average of 250 million Hb molecules • Each Hb molecule has 4 oxygen binding sites • That’s about 1 billion oxygen molecules per RBC! • CO (carbon monoxide) has approximately 200 times the affinity for Hb than oxygen and it can fool O2 saturation detectors
Hemoglobin Structure • Complex quaternary structure Figure 19–3
Fetal Hemoglobin • Strong form of hemoglobin found in embryos • Takes oxygen from mother’s hemoglobin Carbaminohemoglobin • With low oxygen (peripheral capillaries): • hemoglobin releases oxygen • binds carbon dioxide and carries it to lungs Anemia - Hematocrit or hemoglobin levels are below normal - Is caused by several conditions
Recycling RBCs Figure 19–4
Fate and Destruction of Erythrocytes • The life span of an erythrocyte is 100–120 days • Travels about 750 miles in that time (LA to Albuquerque) • Old erythrocytes become rigid & fragile, & their Hgb begins to degenerate • Dying erythrocytes are engulfed by macrophages • Heme and globin are separated • Iron is removed from the heme and salvaged for reuse • Stored as hemosiderin or ferritin in tissues • Transported in plasma by beta-globulins as transferrin • Heme is degraded to a yellow pigment called bilirubin • Liver secretes bilirubin into the intestines as bile • Intestines metabolize bilirubin into urobilinogen • Urobilinogen leaves the body in feces, in a pigment called stercobilin • Globin is metabolized into amino acids which are then released into the circulation
Stimulating Hormones • Erythropoietin (EPO) • Also called erythropoiesis-stimulating hormone: • secreted when oxygen in peripheral tissues is low (hypoxia) • due to disease or high altitude
Diagnosing Disorders • Hemoglobinuria: • hemoglobin breakdown products in urine due to excess hemolysis in blood stream • Hematuria: • whole red blood cells in urine due to kidney or tissue damage
Anemia: Insufficient Erythrocytes • Hemorrhagic anemia – result of acute or chronic loss of blood • Hemolytic anemia – prematurely ruptured erythrocytes • Aplastic anemia – destruction or inhibition of red bone marrow Anemia: Decreased Hemoglobin Content ● Iron-deficiency anemia results from: - A secondary result of hemorrhagic anemia - Inadequate intake of iron-containing foods - Impaired iron absorption ● Pernicious anemia results from: - Deficiency of vitamin B12 - Lack of intrinsic factor needed for absorption of B12 →Treatment is intramuscular injection of B12
Anemia: Abnormal Hemoglobin • Thalassemias – absent or faulty globin chain in hemoglobin • Erythrocytes are thin, delicate, and deficient in hemoglobin • Sickle-cell anemia – results from a defective gene coding for an abnormal hemoglobin called hemoglobinS (HbS) • HbS has a single amino acid substitution in the beta chain • causes RBCs to become sickle-shaped in low oxygen situations
Polycythemia • Polycythemia – excess RBCs that increase blood viscosity • Three main polycythemias are: • Polycythemia vera • Secondary polycythemia • Blood doping
Erythropoietin Mechanism Imbalance Start Normal blood oxygen levels Stimulus: Hypoxia due to decreased RBC count, decreased availability of O2 to blood, or increased tissue demands for O2 Imbalance Increases O2-carrying ability of blood Reduces O2 levels in blood Erythropoietin stimulates red bone marrow Kidney (and liver to a smaller extent) releases erythropoietin Enhanced erythropoiesis increases RBC count Figure 17.6
RBC Tests Table 19–1
Human Blood Groups • RBC membranes have glycoprotein antigens on their external surfaces • These antigens are: • Unique to the individual • Recognized as foreign if transfused into another individual • Promoters of agglutination and are referred to as agglutinogens • Presence or absence of these antigens is used to classify blood groups • Humans have 30 varieties of naturally occurring RBC antigens • The antigens of the ABO and Rh blood groups cause vigorous transfusion reactions when they are improperly transfused • Other blood groups (M, N, Dufy, Kell, and Lewis) are mainly used for legalities
ABO Blood Groups • The ABO blood groups consist of: • Two antigens (A and B) on the surface of the RBCs • Two antibodies in the plasma (anti-A and anti-B) • An individual with ABO blood may have various types of antigens and spontaneously preformed antibodies • Agglutinogens and their corresponding antibodies cannot be mixed without serious hemolytic reactions • FOUR BASIC BLOOD TYPES:
Blood Plasma Antibodies • Type A: type B antibodies • Type B: type A antibodies • Type O: both A and B antibodies • Type AB: neither A nor B
ABO Blood Groups Table 17.4
Rh Blood Groups • Also called D antigen • Presence of the Rh agglutinogens on RBCs is indicated as Rh+; 85% of population is + • Lack of antigen indicated as Rh -; 15% of population. • Anti-Rh antibodies are not spontaneously formed • However, if an Rh– individual receives Rh+ blood, anti-Rh antibodies form • A second exposure to Rh+ blood will result in a typical transfusion reaction • Therefore, only sensitized Rh— blood has anti-Rh antibodies • Hemolytic Disease of the Newborn: Rh- mom pregnant with an Rh+ fetus→ momforms anti-Rh antibodies During next pregnancies: Anti- Rh+ antibodies sensitized Rh– mother cross the placenta and attack and destroy the RBCs of an Rh+ baby The drug RhoGAM can prevent the Rh– mother from becoming sensitized Treatment of hemolytic disease of the newborn involves pre-birth transfusions and exchange transfusions after birth
Transfusion Reactions/Cross Reactions • Transfusion reactions occur when mismatched blood is infused • Donor’s cells are attacked by the recipient’s plasma agglutinins causing: • Diminished oxygen-carrying capacity • Clumped cells that impede blood flow • Ruptured RBCs that release free hemoglobin into the bloodstream • Circulating hemoglobin precipitates in the kidneys and causes renal failure • Blood Type/ Cross MatchTest – determines blood type & compatibility
Leukocytes/ White Blood Cells (WBCs) Do not have hemoglobin ; Have nuclei & other organelles ; complete cells WBC Functions: • Defend against pathogens • Remove toxins and wastes • Attack abnormal cells Most WBCs are in connective tissue proper & lymphatic system organs Small numbers in blood: 6000 to 9000/microliter→ Circulating WBCs - Migrate out of bloodstream via diapedesis - Move through tissues via amoeboid movement - Attracted to chemical stimuli (positive chemotaxis) - Some are phagocytic: neutrophils, eosinophils, and monocytes Leukocytosis – WBC count over 11,000/mm3 - Normal response to bacterial or viral invasion Leukopenia - a decrease in WBC count below 4,800/mm3 Leukemia - a cancer of WBC
Emigration & Phagocytosis in WBCs • WBCs roll along endothelium, stick to it & squeeze between cells. • adhesion molecules (selectins) help WBCs stick to endothelium • displayed near site of injury • molecules (integrins) found on neutrophils assist in movement through wall • Neutrophils & macrophages phagocytize bacteria & debris • chemotaxis of both • kinins from injury site & toxins
5 Types of WBCs Granulocytes: Neutrophils, Eosinophils, Basophils Agranulocytes: Monocytes, Lymphyocytes Figure 19–9
lymphocyte basophil eosinophil monocyte neutrophil
Granulocytes – neutrophils, eosinophils, basophils Contain cytoplasmic granules that stain specifically (acidic, basic, or both) with Wright’s stain Are larger and usually shorter-lived than RBCs Have lobed nuclei Are all phagocytic cells
Neutrophils – Polymorphonuclear Leukocytes (PMNs) • 50–70% of circulating WBCs • Nuclei = 2 to 5 lobes connected by thin strands • older cells have more lobes • young cells called band cells because of horseshoe shaped nucleus (band) • Pale cytoplasm granules (lilac shade) with: • lysosomal enzymes • bactericides (hydrogen peroxide and superoxide) • Fastest response of all WBC to bacteria; 1st to attack bacteria • Engulf pathogens • Digest pathogens • Release prostaglandins and leukotrienes • Form pus Degranulation - removing granules from cytoplasm • Defensins: peptides from lysosomes :attack pathogen membranes
Eosinophils/Acidophils • 2–4% of circulating WBCs • Attack large parasites • Excrete toxic compounds: • nitric oxide • cytotoxic enzymes • Eosinophils account for 1–4% of WBCs • Have red-staining, bilobed nuclei connected via a broad band of nuclear material (but can be 3 lobes) • Have red to crimson (acidophilic) large, coarse, lysosome-like granules • Granules do not obscure the nucleus • Lead the body’s counterattack against parasitic worms • Lessen the severity of allergies by phagocytizing Ag-Ab complexes • Leave capillaries to enter tissue fluid • Release histaminase • slows down inflammation caused by basophils
Basophils • Are less than 1% of circulating WBCs (usually 0.5%) • Have U- or S-shaped bilobed nuclei with two or three conspicuous constrictions • Have large, purplish-black (basophilic) granules that obscure the nucleus • Accumulate in damaged tissue Basophil Actions : • Involved in inflammatory and allergy reactions • Leave capillaries & enter connective tissue as mast cells • Release heparin, histamine & serotonin • heighten the inflammatory response and account for hypersensitivity (allergic) reaction • Histamine: – inflammatory chemical that acts as a vasodilator and attracts other WBCs (antihistamines counter this effect) • Heparin: • prevents blood clotting
Lymphocytes and Monocytes: Lack visible cytoplasmic granules Are similar structurally, but are functionally distinct and unrelated cell types Have spherical (lymphocytes) or kidney-shaped (monocytes) nuclei Agranulocytes