Download

1 / 40
400 likes | 736 Views
贯声门癌组织病理学研究和临床 Histopathological Research of Transglottic Carcinoma. 同济大学附属同济医院 耳鼻咽喉头颈外科 葛荣明 Rongming Ge Tongji Hospital of Tongji University,Shanghai. Transglottic carcinoma. Leroux-Robert(1936) 最初描述 McGavran MH(1961) 首次命名 Tucker GF(1962) 提出声门旁间隙 Kirchner JA(1974) 建议归入分型

E N D
贯声门癌组织病理学研究和临床Histopathological Research of Transglottic Carcinoma 同济大学附属同济医院 耳鼻咽喉头颈外科 葛荣明 Rongming Ge Tongji Hospital of Tongji University,Shanghai
Transglottic carcinoma Leroux-Robert(1936)最初描述 McGavran MH(1961)首次命名 Tucker GF(1962)提出声门旁间隙 Kirchner JA(1974)建议归入分型 吴学愚(1980)百科全书手术谈到 葛荣明(1981)国内首次组织病理证实 费声重、葛荣明(1986)作专题讨论 萧轼之(1989)专著引证采用 黄鹤年(1995)教科书采纳应用
喉解剖冠位、矢位模式图 三区真正交界点在哪里?
除声门上型、声门型和声门下型外,在PGS直接跨越二区者如何归类?除声门上型、声门型和声门下型外,在PGS直接跨越二区者如何归类?
Coronal topographic model about relationships of paraglottic space. 声门旁间隙
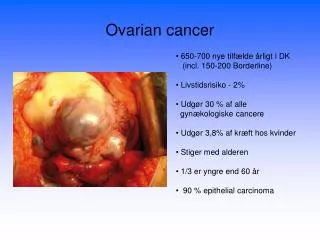
Surgical specimen from a total laryngectomy which showed a characteristic transglottic growth.
TGC is characterized by invasion of the paraglottic space. It invaded thyroid ala leterally and destroyed cricothyroid membrane inferiorly. Superficial mucosa of glottic area is relatively intact (serial section, HE dyeing, coronal site).
The model showed the direction of extension of supraglottic carcinoma. 声门上型喉癌
The model showed the direction of extension of glottic carcinoma. 声门型喉癌
Supraglottic carcinoma invaded into glottic and subglottic area from epiglottis, superficial mucosa of vocal cords were relatively intact.If it was managed by a horizontal supraglottic laryngectomy,the tumor would have been remained
Supraglottical tumor had not invaded glottic area although it was large enough to invade preepiglottic space
An another section of laryngeal specimen was similar to thereinbefore in the same region of tumor
The tumor of laryngeal surface of epiglottis had already invaded preepiglottic space by small holes of epiglottis,but had not reached to the anterior commissure anteroinferiorly.
Supraglottic carcinoma could not invade glottic area in the ventricle laterally because of the effects of the barriers.
TGC destroyed the thyroid cartilage laterally in PGS and invaded both the supraglottic and infraglottic divisions of the larynx.
Transglottic carcinoma 诊断标准: 癌主体在喉室粘膜下为中心向声门旁间隙上下或周围扩展,纵跨两个或以上解剖区,无论其大小,可诊断为TGC
96例TGC病理特点 • 癌生长方式浸润性生长占72% • 扩展广泛性 声带固定 (98%) 侵及会厌前间隙(82%) 破坏喉骨架 (45%) 侵及环甲膜 (34%) 穿过梨状窝达下咽(21%) ﹥2CM的TGC癌瘤侵及喉骨架、扩展至喉外、以及颈转移的比率高
TGC在PGS生长扩展的特点 声门旁间隙(Paraglottic Space, PGS)的界定是: 以喉室粘膜下为中心纵贯两个解剖区的组织间隙 前外 甲状软骨 内侧 喉室和方形膜 内下 弹性圆锥 后界 梨状窝粘膜下 • 肿瘤在PGS增长不受分区界定的限制 • <2.0CM的肿瘤多数在该间隙内 • >2.0CM肿瘤易突破PGS达喉骨架、喉外,颈转移
TGC —喉癌晚期表现? 局部解剖学新认识 PGS为富有血管、神经的脂肪组织间隙 上内方 与会厌前隙相连续,脂肪可突向甲杓肌之间 前下方 在甲状软骨下缘延伸至喉外 后下方 延伸至喉内肌之间,甚至伸到环杓关节 癌可在PGS广泛扩展,是解剖原因不是晚期病变!!
TGC —喉癌晚期表现? TGC在PGS向外侧方 甲状软骨 上内方 会厌前间隙 前下方 直接出喉 后下方 声带和环杓关节运动 后外方 突破梨状窝扩展至下咽 癌可在PGS广泛扩展,是解剖原因不是晚期病变!!
对TGC是否应该做颈廓清术? PGS脂肪结缔组织血运丰富,喉室粘膜下无屏障对贯声门癌行颈廓清是必要的
UICC TNM分类分期为什么至今未把TGC纳入喉癌分型? 贯声门癌(Transglottic carcinoma) 1.词义本身定位已冠上超越声门的前缀,本无T1期可言 2.临床确有TGC存在,与声门上、声门型T2、T3病变有别 3.TGC已被临床广泛应用,可作为一种特殊类型分型诊断
TGC—手术只有喉全切除吗? 全喉切除并不是处理贯声门癌的唯一术式;若术式选择恰当,既能切净甚至扩展至喉外的肿瘤,还可以保留未被癌瘤侵及的喉健康组织,以达到切净肿瘤、保留喉功能的目的
结 论 1.TGC作为临床一种特殊类型有实际意义 2.PGS局部解剖特点是导致TGC易广泛扩展和颈转移的原因 3.对TGC治疗:手术+颈廓清+术后补充放疗
Thank you for your attention Rongming Ge Department of Otolaryngology Tongji Hospital of Tongji University 389 Xincun Road,Shanghai 200065 E-Mail : RongmingGe@sina.com
国际抗癌协会(UICC) 喉癌TNM 分类分期方案(1997)第五版 喉的分区 一、声门上区喉上部(包括边缘区) 1.舌骨上会厌(包括会厌尖,舌面和喉面) 2.舌会厌襞、喉面 3.杓状软骨,声门上部(不包括喉上区) 4.舌骨下会厌 5.室带(假声带) 二、声门区声带、前联合、后联合。 三、声门下区
组织病理学分级(G) GX组织分级不能确定 G1 高分化 G2 中度分化 G3 低分化
临床分期: O期 TisN0M0 Ⅰ期 T1N0M0 Ⅱ期 T2N0M0 Ⅲ期 T3N0M0;T1,2N1M0 Ⅳ期 A T4N0,1M0;任何T N2M0 Ⅳ期 B 任何T N3M0 Ⅳ期 C 任何T任何N M 1
远处转移部位缩写符号 肺 PUL pulmonary 骨 OSS osseous 肝 HEP hepar 脑 BRA brain 淋巴结 LYM lymph 骨髓 MAR marrow 胸膜 PLE pleura 皮肤 SKI skin 其他 OTH other
国际抗癌协会(UICC) 喉癌TNM 分类分期标准(2002) 喉的解剖分区 一、声门上区 1.舌骨上会厌(包括会厌尖,舌面和喉面) 2.舌会厌襞、喉面 3.杓状软骨 4.舌骨下会厌 5.室带 二、声门区声带、前联合、后联合 三、声门下区
声门上型 T1局限于声门上区的一个亚区,声带运动正常。 T2 侵犯声门上区一个亚区以上、侵犯声门或声门上区以外(舌根黏膜、会厌谷、梨状窝内壁黏膜),无声带固定。 T3肿瘤限于喉内,声带固定和/或侵犯:环后区、会厌前间隙、声门旁隙、和/或伴有甲状软骨局灶破坏(内板) T4a肿瘤侵透甲状软骨板和/或侵及喉外组织(气管、颈部软组织、带状肌、甲状腺、食管等) T4b肿瘤侵及椎前间隙,包裹颈总动脉,或侵及纵隔结构
声门型 T1侵犯声带(可以侵及前或后联合),声带活动正常 T1a肿瘤限于一侧声带 T1b双侧声带受侵 T2向声门上和/或下侵犯,和/或伴声带活动受限 T3肿瘤局限在喉内,声带固定和/或侵犯声门旁间隙,和/或伴有甲状软骨局灶破坏(内板) T4a肿瘤侵透甲状软骨板和/或侵及喉外组织(气管、包括舌骨在内的颈部软组织、带状肌、甲状腺、食管) T4b肿瘤侵及椎前间隙,侵及结构,或包裹颈总动脉
声门下型 T1肿瘤限于声门下区 T2肿瘤侵及声带,声带活动正常或受限 T3肿瘤限于喉内,声带固定 T4a肿瘤侵透环状软骨或甲状软骨板,和/或侵及喉外组织(气管、包括舌外肌在内的颈部软组织、带状肌、甲状腺、食管) T4b肿瘤侵及椎前间隙,侵及结构,或包裹颈总动脉
临床分期: O期 TisN0M0 Ⅰ期 T1N0M0 Ⅱ期 T2N0M0 Ⅲ期 T3N0M0;T1,2,3N1M0 Ⅳ期 A T4aN0,1M0;任何T N2M0 Ⅳ期 B 任何T N3M0;T4b任何NM0 Ⅳ期 C 任何T任何N M 1