Download
1 / 21
300 likes | 884 Views
Work of Breathing. Components 1. Compliance work 65% (stretching lungs & chest wall) 2. Airways resistance work 30% 3. Moving tissues 5% Normally <1–3% Total Energy (E) in exercise, still <3–5% total E output. Volume. Compliance =. Pressure. Lung resists stretching:.

E N D
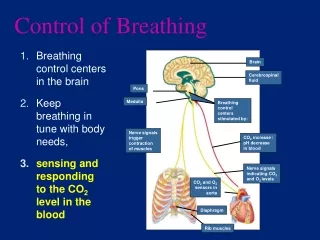
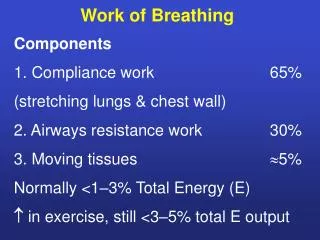
Work of Breathing Components 1. Compliance work 65% (stretching lungs & chest wall) 2. Airways resistance work 30% 3. Moving tissues 5% Normally <1–3% Total Energy (E) in exercise, still <3–5% total E output
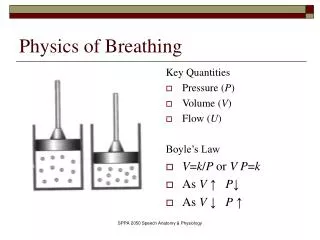
Volume Compliance = Pressure
Lung resists stretching: • Tissue expansion: Small componentnormally Fig. shows lung expansion involves an unfolding of elastin and collagen fibers in the alveolar walls. The actual lengths of the individual fibers change little.
Major component: surface tension dynes / cm
Lung surfactant • protein-phospholipid • from alveolar type 2 cells • Functions • 1. surface tension of fluid in alveoli, so lungs able to expand with normal muscle activity. • 2. Stabilizes alveoli from collapse • surface tension is lowered more in small alveoli than in larger alveoli • P = 2T • r
Small alveolus surfactant molecules more concentrated Large alveolus surfactant molecules more diluted Fig. shows surface tension alters alveoli stability. The smaller alveoli generate a greater pressure and cause air to flow into larger units. Surfactant promotes alveolar stability by lowering surface tension proportionately more in the small alveoli.
Compliance work 1. where surfactant ~ premature babies (smoking) 2. where lung tissue fibrotic (scar tissues) ~ coal miners ~ asbestosis 3. where chest wall expansion limited ~ scoliosis ~ tight bandages 4. at high lung volumes
compliance work Fig. shows static expiratory pressurevolume curves of lungs in normal subjects and subjects with pulmonary fibrosis.
Airway Resistance pressure gradient Gas flow = resistance 1 with laminar flow resistance 4 radius • Airway resistance is increased by • turbulent flow e.g. rapid breathing • airway narrowing
Small peripheral airways • each has small diameter • but many of them • so total cross-sectional area is high • reactive smooth muscle in wall
Fig. shows schematic representation of airway branching in the human lung with approximate dimensions.
Causes of airway narrowing • in expiration vs inspiration • ~ expiratory forces tend to push airways shut • worse if little support for airways • ~ emphysema = lung tissue destruction floppy airways close during expiration air trapping • smooth muscle constriction e.g. asthma • inflammation, mucus, mucosal swelling • e.g. chronic bronchitis asthma
Airway resistance is affected by: 1. Structure of lungs ~ resistance is higher in upper airways (trachea/bronchi etc) ~ lower in small airways (large total cross-sectional area, laminar flow) 2. Mechanical factors: Airway resistance is in expiration vs inspiration expiratory forces tend to push airways shut worse if little support for airways ~ airway resistance is lower at high lung volumes – airways held open ~ airway resistance is lower during inspiration vs expiration
3. Smooth muscle tone in small airways ~ sympathetic input relaxation ~ parasympathetic input constriction ~ immune response e.g. asthma allergen/cold triggers immune response inflammatory mediators released smooth muscle constriction, mucosal swelling and mucus secretion 4. Local reflexes: Areas with PCO2 cause bronchiolar smooth muscle contraction: important for ventilation-perfusion matching
Mechanical factors cont: ~ airway resistance may be high during expiration due to dynamic airways collapse during expiration (forced expiration, “floppy” airways in emphysema) Emphysema = lung tissue destruction floppy airways close during expiration air trapping
Spirometry Forced expiratory volume in 1 sec F E V1 ~ measure of airways obstruction and/or dynamic airway compression ~ since F E V1 also affected by F V C (forced vital capacity) F E V1 / F V C ratio used N ratio 80%
FEV1 = 3.2L FVC = 4L FEV1 = 1.5L FVC = 3.2L
Overall Work of Breathing 1.Compliance work is greatest at high lung volumes 2. Airways resistance work is greatest at rapid airflow rates ie highest respiratory rate / min minute ventilation VT = VT x resp rate L / min tidal vol
Work of breathing (summary) • Compliance work. • ~ surfactant • measurement: static compliance curve spirometry • ~ airways resistance work • measurement: • alternative: peak flow meter • V P F E V1 F V C