Download
1 / 16
200 likes | 933 Views
MECHANICS OF BREATHING. Dr.M.Kannan MD DA Professor And HOD Department of Anaesthesiology Tiunelveli Medical College. MECHANICS OF BREATHING. Introduction : all about how the lung is supported and moved. Applications during conduct of GA, Intensive care.

E N D
MECHANICS OF BREATHING Dr.M.Kannan MD DA Professor And HOD Department of Anaesthesiology Tiunelveli Medical College
MECHANICS OF BREATHING Introduction : all about how the lung is supported and moved. Applications during conduct of GA, Intensive care. Components of mechanics: 1. Muscles of respiration 2. Compliance 3. Airway resistance 4. Work of breathing
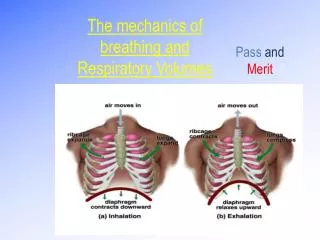
MUSCLES Diaphragm: Abnormalities of movement: a. unilateral phrenic n. palsy. b. Pressure from below c. Upper abdominal surgery d. In advanced emphysema e. In some lung diseases External intercostals: Paralysis/paresis of intercostals=nerve block, extra- dural and sub-arachnoid block, transection of spinalcord, residual neuro-muscular blockade,inanition.
: Accessory muscles: a. The scalene muscles b. The sternocleidomastoid c. Anterior serrati d. The alae nasi e. small muscles of the head and neck. Muscles of expiration: Normally passive. Active during exercise ,forced expiratory manouevers. Mechanism of respiration
PRESSURE-VOLUME RELATION-CHARACTERISTICS non-linear. Curved. Different for inspiration & expiration.Hysteresis present. Compliance: Lung compliance+ chest wall compliance §V/§P(L/cm H2O) §P= Palv-Ppleural(transpulmonary) §P= P pleural-Patm(transmural) a+b=transthoracic§P=Palv-Patm Cl= slope of the curve just described.
In thenormal range of expanding pressures of -2 to -10 cms of H2O, the lung compliance=0.2 L/cm of H2O .However at higher expanding pressures-compliance is less. Measurement of compliance: pressure in the pleural cavity-measured by implanting a balloon tipped catheter in the pleural cavity. Indirectly, oesophageal pressure-can be measured. Alveolar pressure- pressure at the site of airway opening. Lung compliance is ↑ in a. emphysema b. with advancing age (destruction of elastic tissue of the lung.)
Specific compliance: Though the compliance is ↑ in emphysema- the lungs don’t function better mechanically.damage to the elastic fibres-gas trapping occurs-FRC is ↑. The resting ventilation –operating on the flat part of the pressure-volume curve, so during normal tidal breathing-compliance is less. This is specific compliance. Specific compliance= Compliance(L/cm H2O)/Volume of lung at FRC.
Elastic properties of the chest wall Normally, chest wall compliance= lung compliance. Total compliance= lung compliance+chest wall compliance=0.1 L/cm H2O. Factors affecting compliance Lung volume Hysteresis Posture 4. Pulmonary blood volume:
Restriction of expansion of the chest: • IPPV-reduces compliance. • a. by causing uneven ventilation • b. by airway obstruction due to accumulation of cellular debris due to reduced ciliary activity. • GA • Disease states.
Dynamic compliance: First measure peak airway pressure. It is the pressure measured at the airway opening at end- expiration,after subtracting applied CPAP. Cdyn= inspiratory volume/peak airway pressure. Static compliance: If expiration is prevented from occuring following inspiration, the respiratory muscles relax-airway pressure drops. Cstat= inspiratory volume/plateau airway pressure.
Anaesthetic implications • Changes in dynamic compliance without changes in Cstat=↑airway resistance. • Alterations in both dynamic and static compliance=change in lung stiffness.
Surface tension Laplace’s law: P=2T/R. Surface tension kept constant, with reducing radius of the alveoli- retraction pressure would rise-collapse of the smaller alveoli-emptying into the larger alveoli. This does’nt happen due to the presence of surfactant.lipoprotein with phospholipid-dipalmitoyl phosphatidyl choline. Dense molecules in the smaller alveoli-keep the pressure more or less constant. Functions: Application=in neonatal respiratory distress syndrome.
Interdependence:surrounding alveoli exert expanding forces. Regional differences in ventilation: better ventilation of the base and dependent lung. Converse true at low lung volumes. What happens during ageing? AIRWAY RESISTANCE >2/3 of the work=spent in overcoming airflow resistance when RR>50/min Laminar flow: Flow=pir4/8nl Turbulent flow/orificial flow Applications .
Airway resistance-contd. • Airway resistance= mouth pressure-intra-pleural pressure/flow Normal value:0.05-2 cm H2O/l/sec in adults. Variations: • Lung volume • Bronchial muscle tone • Drugs • Posture The response to↑ airway resistance:
Dynamic compression of airways: EPP describes it. • Abnormal expiratory flow rates. • Tissue resistance • Pulmonary resistance
WORK OF BREATHING • Elastic, non-elastic airway work. Work=pressurexvol Normal metabolic cost=1-3% of total O2 Consumption Optimum pattern of ventilation for diseased lungs