Download
1 / 25
250 likes | 259 Views
National Audit of Dementia (care in general hospitals). Partners to the audit. Background. CCQI scoping report for Healthcare Commission 2007: Finding that care of people with dementia in general hospitals is high priority for audit

E N D
Background • CCQI scoping report for Healthcare Commission 2007: • Finding that care of people with dementia in general hospitals is high priority for audit • - In a typical 500 bed general hospital, 20% admissions will have dementia (Who Cares Wins, 2005) • - Hospitals can be ill prepared and care can be inconsistent • - People with dementia experience worsening of condition and poor outcomes
Participation in the audit • Participation in the core audit • 210 or 89% hospitals • 99% Trust participation • 210 checklists • 7934 case notes of people with dementia • Participation in the enhanced audit • 55 hospitals (145 wards) • 144 environmental checklists • 145 ward checklists • 2211 staff questionnaires • 245 patient questionnaires • 608 observations of care interactions
Key findings 6% of hospitals had a care pathway 44% of hospitals had a care pathway in development. Information reviewed by the Executive Board:
Summary Lack of leadership both at Trust/Health Board level and at hospital level. In terms of identifying champions and leads, and identifying required resources. Trust Boards/Health Boards require better intelligence and information on admission, care, treatment and discharge of people with dementia. Improvements can be made to processes and overall governance.
Key findings 13% of casenotes no formal pressure sore risk assessment. 19% of casenotes not asked about any continence needs as part of assessment. 24% of casenotes not asked about any pain as part of the assessment. Summary Gap between policy and practice. Adherence to multidisciplinary assessment procedures should be clarified and reinforced.
Key findings 28% of people with dementia received antipsychotic medication in the hospital.
Summary Widespread provision of liaison psychiatry but lack at evenings and weekends. Likely to impact on the time taken by services to respond to an emergency or urgent referral. A lack of mental health assessment during admission and discharge - mental health needs often overlooked May affect ability to carry out assessment or to see patients who require onward referral for diagnosis. Hospitals should ensure challenging behaviour is managed with awareness and understanding, guidelines are reviewed and training for staff is in place. If antipsychotic medication prescribed, a reason should be recorded and it should be reviewed regularly.
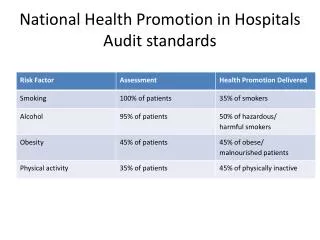
Summary • Much could be done at hospital level and ward level to improve nutritional standards: • Standardised assessment and recording of weight over time. • Support to assist patients at mealtimes. • Making food available at other times. • Implementation of protected mealtimes.
Summary • Lack of guidance in hospitals for involving families in discharge and support arrangements Families not routinely involved in care and often not given named healthcare professional to contact for help. • Ward systems for recording and communicating basic personal information about patients with dementia This information not a systematic part of assessment.
Summary Patients’ families/carers not asked about behaviours that may indicate distress or useful strategies to help the patient feel safe and calm. This information could reduce the behaviour disturbance and avoid antipsychotic medication. Hospitals need clear guidelines on information to be collected, and on supporting staff to share and use information and involve carers
Summary 96% of staff agreed further training on dementia awareness needed to improve the care people with dementia receive. Comments on particular aspects of care reveal that further training is needed across all job roles for a range of competencies related to the care of people with dementia.
Summary The experience of people with dementia could be improved by attention to orientation both in the ward (signage, use of colour) and the bed area (positioning of familiar personal items) use of space to provide breaks from the ward environment Evidence from observations of care also suggested that attention to noise and creating a warm, friendly atmosphere are important in the care of people with dementia
Key findings - casenotes 67% up-to-date discharge plan. 58% evidence that support needs identified in the discharge plan. Only 41% showed a copy of the plan passed on to patients or carers. 75% assessment of the carer’s current needs had taken place before discharge. 80% place of discharge and support needs discussed with carer/relative.
Summary It is encouraging that: Most casenotes show evidence of attention to the carers’ needs most showed involvement of the carer in discharge and support. But: in half the casenotes discharge planning had not begun at admission, for no stated reason. half had no named discharge co-ordinator Early discharge planning helps timely discharge and reduces time spent by the person with dementia in the acute environment - cost savings
Training and communication • 5% hospitals said that dementia training • (care provision, systems, information and resources available in the hospital) mandatory for all healthcare staff • 16% hospitals said training was available not mandatory for all staff or some key staff • Over 90% of all staff agreed further training would improve the level of care received by people with dementia
Key findings On most hospital wards there is little evidence of a person-centred ward approach or ‘culture’, or that the care received by patients is generally person-centred. The content of the staff/patient encounter is mainly task related and delivered in an impersonal manner. Periods of care-based activity interspersed with inactivity leading to lack of attention, lack of stimulation and boredom for patients. Environment is often impersonal and not dementia friendly excess noise at times, lack of orienting cues, no areas for socialising.
Information on the ward – staff comments Staff comments: “These systems are in place, but due to high numbers of agency staff that are unfamiliar with documentation these systems are not always effective” “Although staff do communicate with one another I feel there is lacking handover information especially to nursing assistants” “A minimal handover is given with the most basic of information, due to cutting time. Extra information is ideal but not realistic on this ward” “We now have a booklet on the ward for patients and/or family to fill in to help.” “There is NO WAY EVER enough time to collect or even read the personal information for the patient”
Information and communication - observations • About half of the wards identified this as an area in need of improvement • One patient had preferences to his drinks (like and dislikes), staff ensured he had his favourites at hand (this was important as his oral intake needed encouragement).’ • Feedback noted where improved communication could have anticipated and prevented problems: • Not all staff were aware of personal preferences in terms of patient care/choices e.g. likes and dislikes in diet and drinks. One patient reported they liked their water warm, staff brought a glass of cold water, the patient said they liked warm water and the water was cold and couldn’t take their medicine.
Improving quality of care • Local reporting shows comparison with national level data on each of the criteria • Hospitals were asked to produce action plans • Wards participating in observation highlighted areas for celebration and improvement • National report made recommendations for improvement and focused on identified good practice • A second round of audit begins in Spring 2012 - this repeats hospital audit • A new project, the Quality Mark for Elder-Friendly care, is in development, and will build on the results of the ward level audit
A call to action from you! Urgent need for research to find a cure for Alzheimer’s and other forms of dementia Developing prevention of a cure and getting it into widespread use could take 10, 20 or even 30 years There is also an urgent need to improve dementia care now Audits and service improvements are useful but limited Need to support research to improve dementia care - develop interventions, what works, what’s cost effective? In last few years Dept of Health funding for dementia care research has increased significantly Alzheimers Research UK and Alzheimers Society 113 projects and only 8 (7%) on improving care Action needed from DAA to value, encourage and support dementia care research