Download
1 / 23
230 likes | 248 Views
This case study follows a seven-year-old stallion with a history of renosplenic entrapment and laparoscopic renosplenic space ablation. The horse presented with signs of colic and was non-responsive to analgesia. Emergency diagnostics, including rectal palpation and trans-abdominal ultrasound, confirmed the recurrence of renosplenic entrapment. The possible causes of failure of the initial ablation procedure are discussed. Medical treatment options, including phenylephrine and exercise, are explored.

E N D
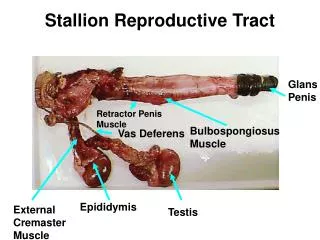
RECURRENCE OF RENOSPLENIC ENTRAPMENT FOLLOWING RENOSPLENIC SPACE ABLATION IN A STALLION Emily A. Barrell, MS Mentors: Dean A. Hendrickson, DVM, DACVS; J. Lacy Kamm, DVM Colorado State University Veterinary Teaching Hospital Fort Collins, Colorado
SIGNALMENT AND HISTORY •“Christian Geronimo” •Seven-year-old Appaloosa-Trakehner stallion • Previous history of renosplenic entrapment and laparoscopic renosplenic space ablation 7 years prior as a weanling • Referred in October 2009 for signs of colic: -Inappetance -Rolling -Decreased defecation •Non-responsive to analgesia as per rDVM (xylazine, butorphanol, buscopan, ephedrine)
CLINICAL FINDINGS On presentation, horse was sweating, shaking, and uncomfortable Physical exam findings:
EMERGENCY DIAGNOSTICS 1. RECTAL PALPATION: Normally palpable structures: Abnormal findings: Pelvic flexure Cecal distension Parts of ventral & dorsal colon Distended small intestine Cecum Distended large or small colon Mesenteric root in small horses Bowel edema Iliac arteries & descending aorta Mesenteric edema Small colon w/fecal balls Malpositioned bowel Spleen Impaction Left kidney Intussusception Renosplenic ligament and space Mass/abscess Bladder Mesenteric root volvulus Results in this case: Left colon positioned dorsal to spleen Left kidney and renosplenic ligament could not be palpated
EMERGENCY DIAGNOSTICS 2. TRANS-ABDOMINAL ULTRASOUND: Place probe in 15th – 17thintercostal space parallel to the adjacent ribs It may be necessary to image more ventral than normal to visualize the dorsal border of the spleen if renosplenic entrapment is suspected as the colon can push the spleen ventrally
EMERGENCY DIAGNOSTICS 2. TRANS-ABDOMINAL ULTRASOUND: Other findings that may mimic renosplenic entrapment: non-specific large colon distension, small intestine in the renosplenic space (normal finding) Results in this case: Left kidney could not be visualized as colon was dorsal to the spleen Ventrally deviated spleen with rounded margins -Enlargement of the spleen is common with renosplenic entrapment due to the colon inducing splenic congestion via pressure on the vasculature Spleen Spleen Large colon Left kidney Normal Abnormal (Renosplenic entrapment)
EMERGENCY DIAGNOSTICS 3. ABDOMINOCENTESIS: Normal values: TP < 2.0 g/dl; WBC < 5000 cells/µl; Clear, straw-yellow color Common abnormalities: Large intestinal obstruction: TP > 2.0; WBC variable Strangulating small intestinal lesion: TP > 4.0; WBC variable; serosanguinous color Renosplenic entrapment: TP and WBC often normal →Increased TP or WBCs can indicate longer duration of entrapment and may make surgical correction more likely Results in this case: Abdominal fluid slightly serosanguinous TP = 1.3 g/dl
PROBLEM LIST • Pale mucus membranes • Delayed CRT • ↑ PCV • Tachycardia • ↓ Gut sounds* • Colic/Abdominal pain* • Ventrally deviated spleen* • Displaced left colon* • Non-visible left kidney on ultrasound* Hypovolemia * Denote most significant problems
DIFFERENTIAL DIAGNOSES Moderate Abdominal Pain - Non-strangulating obstruction - Colitis - Displaced colon Displaced left colon -Renosplenic entrapment -Gas colic -Large colon torsion Ventrally deviated spleen - Renosplenic entrapment Non-visible left kidney on u/s - Renosplenic entrapment - Fluid- or gas-distended large colon - Small intestine or small colon in the renosplenic space ↓Gut sounds - Reduced feed intake - Ileus - Obstruction
DIAGNOSIS Based on: Rectal exam findings Ultrasound imaging Abdominocentesis Clinical presentation Top differential is RENOSPLENIC ENTRAPMENT, despite a previous renosplenic space ablation procedure Prior to this case, recurrence of renosplenic entrapment following a renosplenic space ablation has NOT been reported
POSSIBLE CAUSES OF FAILURE Possible causes of failure of the initial renosplenic space ablation: •Young age of colt at time of first procedure -Shape or size of renosplenic space may change with age, causing the ablation to fail •Inadequate suture bite size and spacing through the visceral peritoneum and splenic capsule -Too much tension along suture line may cause the ablation to fail
MEDICAL TREATMENT OPTIONS Phenylephrine - Alpha adrenergic agonist - Causes splenic contraction - Up to 90% success rate in stable patients - Dose: 8-16mg/450kg in 1L saline given over 15 minutes - Heart rate and rhythm should be monitored during administration - Can be repeated several times CAUTION: Do not administer to hypovolemic patients as reflex bradycardia may ensue and result in hypoperfusion
MEDICAL TREATMENT OPTIONS Exercise - Jogging for 15-30 minutes to shake the colon loose from the renosplenic space -Repeat rectal exam after exercise to evaluate position of the colon Rolling -General anesthesia is used to place horse in dorsal recumbency while abdomen is vigorously balloted -Horse can then be placed into left lateral, balloted again, and rolled to right lateral recumbency for recovery COMPLICATIONS: Cecal or colonic volvulus (iatrogenic) Cecal or colonic rupture Persistence or worsening of left displacement ROLLING VIDEO
SURGICAL TREATMENT OPTIONS • 1. Ventral midline celiotomy • Advantages: • Access to majority of anatomy • Correction of unexpected/undiagnosed findings • Disadvantages: • Requires general anesthesia • Longer convalescent period • Increased cost to owner • When to use: • Evidence of intestinal compromise • Evidence of other intestinal lesions • Inability to perform a rectal exam pre-operatively • Inability to adequately control pain without general anesthesia
SURGICAL TREATMENT OPTIONS 2. Standing flank laparotomy Advantages: Avoidance of general anesthesia Direct access to affected anatomy Option for simultaneous closure of renosplenic space Reduced convalescent period Reduced cost to owner Disadvantages: Limited access to other anatomy in the case of incorrect diagnosis or multiple lesions
METHODS FOR PERMANENT CORRECTION •Colopexy •Large colon resection •Surgical closure of the renosplenic space →Open vs. laparoscopic →Suture closure vs. mesh placement
THERAPEUTIC PLAN • Phenylephrine + exercise • →Horse was administered phenylephrine and • jogged, but rectal exam showed no resolution of • entrapment • Rolling and abdominal ballottement under general anesthesia • →Horse was anesthetized and placed in dorsal recumbency with hindlimbs hoisted. Abdomen was balloted and horse was placed in left lateral recumbency for recovery. Rectal palpation following recovery confirmed resolution of the entrapment • Surgical correction if necessary • →Unnecessary in this case • Repeat renosplenic space ablation • →Scheduled approximately 2 weeks after discharge
THERAPEUTIC PLAN Repeat laparoscopic renosplenic space ablation Laparoscopy sites – left flank: Instrument portal Paralumbar fossa midway between 18th rib and tuber coxae Laparoscope portal 17th Intercostal space, level with dorsal tuber coxae Large-bore cannula portal 5cm ventral to instrument portal Cranial Caudal
REPEAT RENOSPLENIC ABLATION Necropsy photo of a horse that had a renosplenic space ablation 3 years prior. Note the complete and smooth fibrous adhesion (large arrow) joining the spleen (asterisk) and perirenal fascia. The renosplenic ligament is denoted by the small arrow. Laparoscopic view through Christian’s left 17th intercostal space looking caudally, 7 years following the initial renosplenic space ablation. Where there should be continuous fibrous coverage of the space, only four bands of adhesion remain.
REPEAT RENOSPLENIC ABLATION Renosplenic space was closed once again - Splenic capsule sutured to visceral peritoneum - Autologous blood from suture placement may serve as a source of fibrin Perirenal fascia Spleen
OUTCOME “Christian” discharged from the hospital and recovered well at home Five months following the procedure owner reports no recurrences or complications
FURTHER READING/REFERENCES 1. Epstein KL, ParenteEJ. Laparoscopic obliteration of the nephrosplenic space using propylene mesh in five horses. Vet Surg. 2006; 35:431-437. 2. Farstvedt E, Hendrickson DA. Laparoscopic closure of the nephrosplenic space for prevention of recurrent nephrosplenic entrapment of the ascending colon. Vet Surg. 2005;34:642-645. 3. Mariën T. Laparoscopic closure of the nephrosplenic space in the standing horse. In: Equine diagnostic and surgical laparoscopy. Ed: Fischer AT; W.B. Saunders Company, Philadelphia. 2002. Pp. 265-271. 4. Mueller POE, Moore JN. Gastrointestinal emergencies and other causes of colic. In: Equine emergencies: treatment and procedures, 3rd ed. Ed: Orsini JA, Divers TJ; Saunders Elsevier, Saint Louis. 2008. 5. Rakestraw PC, Hardy J. Large intestine. In: Equine surgery, 3rd ed. Ed: Auer JA, Stick JA ; Saunders Elsevier, Saint Louis. 2006. Pp. 453-456.
ACKNOWLEDGEMENTS Photographs courtesy of Dr. Dean Hendrickson, Dr. Diana Hassel, Ms. Alisa Blake, and Mr. Ron Wahl. Thanks to Dr. Hendrickson, Dr. Lacy Kamm, and Dr. Hassel for all their time and assistance