Miami
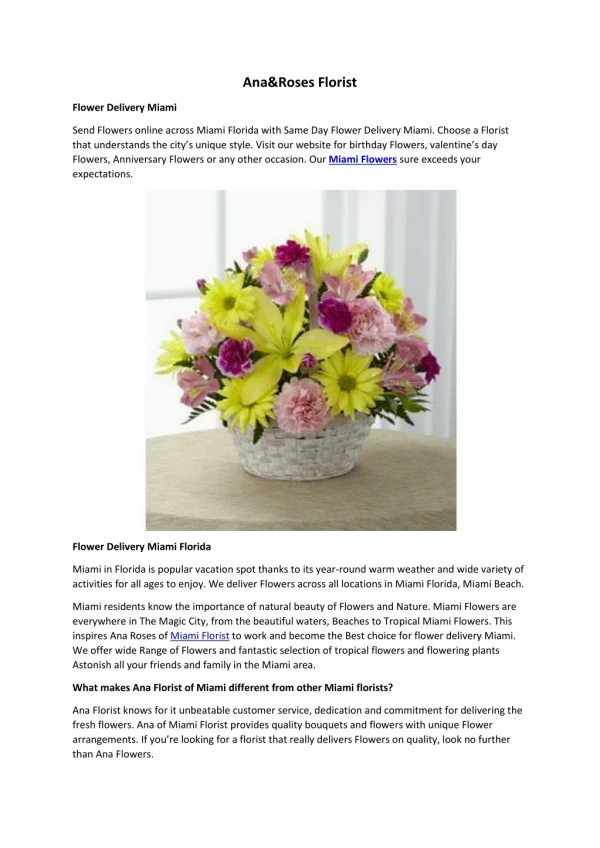
Miami. UNIVERSITY OF. SCHOOL OF MEDICINE. Immunology and Infection in Chronic Fatigue Syndrome. Nancy Klimas, MD. Miami VAMC. Model of CFS Pathogenesis. Genetic Predisposition Triggering event / infection

Miami
E N D
Presentation Transcript
Miami UNIVERSITY OF SCHOOL OF MEDICINE Immunology and Infection in Chronic Fatigue Syndrome Nancy Klimas, MD Miami VAMC
Model of CFS Pathogenesis Genetic Predisposition Triggering event / infection Mediators (Immune, endocrine, neuroendocrine, psychosocial, viral reactivation or persistence) CFS/ME
Genetic Predisposition - CFS • HLA DR haplotypes in 112 South Florida CFS patients, compared to 5,000 regional and national controls • 4 to 6 fold increased relative risk for DR4, DR3 and DQ3. (Keller et al, 1992) • Seattle CFS Cooperative Research Center Twin study - genetic predisposition, hereditability estimate of 51% (2nd World Conf); similar results in Sweden, Australian studies
Evidence for Triggering event/ infection - CFS • 60 to 80% of CFS subjects onset an acute viral-like illness (Komaroff, Buchwald) Less so in population based studies. (Reeves, Jason) • Andrew Lloyd and colleagues in Australia performed a prospective study - anergy during acute infection predicted persistent CFS like symptoms • Severity of initial infection single best predictor
Model of CFS Pathogenesis Genetic Predisposition Triggering event / infection Mediators (Immune, endocrine, neuroendocrine, psychosocial, viral reactivation or persistence) CFS/ME
CRF • CNS Symptoms • Altered perceptions • fatigue • pain • Cognitive changes • concentration • memory • Mood alterations • depression • anxiety • Sleep disturbances • unrefreshing sleep • altered sleep-wake cycle Physical stress activates immune system and HPA axis Emotional stress activates immune system and HPA axis • Hypothalamic-Pituitary-Adrenal Axis • Relative Hypocortisolemia • Musculoskeletal System • Myalgia & Arthralgia • Gastrointestinal Tract • Altered bowel habits • Abdominal pain • Heart and Blood Vessels • Altered blood pressure • responses • Dizziness • Immune System • Lymph node tenderness • Sore throat • Enhanced Cytokines
Video link: The leukocyte • . http://www.studiodaily.com/main/searchlist/6850.html http://multimedia.mcb.harvard.edu/media.html
Immune Activation DR, CD26 expression TH2 cytokine shift Proinflammatory cytokines expression TNF-a, IL-1, IL6 Functional defects NK Cell dysfunction CD8 abnormalities perforins, granzymes Macrophage abnormalities Antibody production Immune abnormalities in CFS
40 35 30 25 GWI 20 CFS 15 Controls 10 5 0 Subjects NK Cytotoxicity: % K562 Cells Killed at Target to Effector Cell Ratio of 1:1
Natural Killer Cell Cell Surface Antigen: CD56 Intracellular Cytolytic Granules: * Perforin * Granzyme A * Granzyme B Perforin is a molecule in cytotoxic lymphocytes necessary for killing of virus infected and tumor cells.
Natural killer (NK) cell cytolytic capacity was measured by quantitative flow cytometry of intracellular content of perforin, with data expressed as relative number of molecules of perforin per CD3-CD56+ lymphocyte (rMolPer/NK cell).
7000 6000 5000 4000 GWI CFS 3000 Controls 2000 1000 0 Subjects Intracellular Perforin
CD26 (dipeptidyl peptidase IV) is involved in the activation of T cells, and is expressed on antigen-reactive memory T cells. As reported by the Miami CFS research group, the percentage and number of CD26+ lymphocytes is elevated in CFS.
70 60 50 40 GWI CFS 30 Controls 20 10 0 Subjects Lymphocyte Activation in GWI and CFS: Percent of CD2+CD26+ Lymphocytes Fig. 3. Lymphocyte Activation in GWI and CFS: Percent of CD2+CD26+ Lymphocytes
Qualitative flow cytometry showed fewer numbers of molecules of DPPIV/CD26 on T and NK cells in CFS patients.
Neuropeptide-Y (NPY) is peptide,which participates in the regulation of a large number of physiological and pathophysiological processes in the cardiorespiratory system, immune system, nervous system and endocrine system. NPY is stored in sympathetic nerve terminals and is released along with catecholamines during stress-induced activation. Only a few peptidases are capable of cleaving NPY due to its unique 3-diminsional structure. DPPIV/CD26 is one such peptidase.
In the GWI patients, we found a reduced amount of NPY in plasma. *Significantly different from HC (p<.05)
. .. .
. . .
Paced Auditory Serial Addition Task (PASAT) Women with CFS 55 p = <.001 41 28 14 Low NKCC Normal NKCC n = 22 n = 19 0 The PASAT is an objective measure of: Group Means (+/- SD) rate of information processing, sustained attention and dividedattention
Immune –Endocrine Link IL-6 increase associates with low cortisol, CRH mediated Papanicolau Neuroimmunomodulation 2004 11(2)65-74 Maes M Neuro Endocrinol Lett 2005 Oct 30;26(5)
Viral Persistence/Reactivation HHV6 virus is present in 22 to 54% of patients in cross sectional studies (Ablashi, Krueger, Knox), HHV6 virus is present in 79% of CFS patients in longitudinal studies (HHV6 PCR assay, Knox) HHV6 virus is present in the spinal fluid of 28 of 120 CFS patients (Peterson), and 7 of 35 CFS samples (Knox). Enterovirus is present in 13% of CFS muscle samples (Douche-Aourik, 2003); EBV – dUTPase as a immune modulator, up regulating inflammatory cytokines (Glaser, 2005) (Glaser et al Brain Behavior and Immunity 2005 19(2):91-103)
Viral and Immune Interactions and Health • J Chia showed GI biopsies with enterovirus inclusions, found in patients with CFS and abdominal complaints
Novel mechanisms of virus mediated chronicity • Glaser et al found evidence of regulatory peptides encoded by EBV expressed in CFS despite the absence of replicative virus • These peptides are known to modulate immune function, inducing pro-inflammatory and Type 2 cytokines • Lerner’s group found evidence of a subgroup of CFS patients with incomplete viral expression and cardiac motility abnormalities; subset of CFS with IgM EBV 2 Lerner M et al In Vivo 2004(18) 4:417; (18)2:101 3 Glaser R Brain Behavior Immun 2005 19(2):91
Treating HHV6a?Association vs. causation • Blood PCR HHV6 a did not predict HHV6 virus is present in the spinal fluid • CSF did not predict blood • Of 120 CSF samples, 44 had abnormalities of protein, glucose or cells. Of the 44 , 28 were positive for HHV6(26), EBV (1), or CMV(1). • 5 of 8 CSF PCR positive treated until CSF cleared returned to full time employment (Peterson); in his experience TK inhibitors did not clear CSF, patients required foscarnet or cidofovir • Open label valgancyclovir 20 of 23 responders in high titer EBV plus HHV6 selected cohort , (Jose Montoya) • Placebo control trials have not been completed
Clinical Trials • M Lerner reported a phase 1 trial of valgangciclovir in CFS patients with evidence of cardiac dysfunction. 37 patients were treated in an open label study, with improvement in all 37. He emphasized the need to hydrate, monitor renal and liver function.
Genomics, Proteomics, and Viral Chips • IACFS Conf 2007 : • Inflammation pathways, IL-6, TNFa upregulated in a subgroup, suggesting monoconal ab blockers as a treatment (Kerr, Vernon, Olano) • CFS proteome (Baruniuk) • Serum analysis using infrared spectroscopy (Sakudo, Watanabe, Ikuta, Kuratsune) • 28 potential microbes under study (Kerr) • Reno research group using viral chip technology in CFS and CFS associated malignancy
Conclusion • Immune dysfunction in CFS contributes to the overall symptom complex, and contributes to the persistence of the illness, both directly and through interaction with neuropeptides and hormones. • There is increasing evidence of viral reactivation in at least a subset of the patient population. Interventive trials are currently focused on HHV6 virus. • This work is helping to identify subgroups of CFS patients, identifying biomarkers, and potential treatment options.
Thank You! Immunology/Virology: Drs. Mary Ann Fletcher, Kevin Maher, Roberto Patarca Autonomic: Dr. Barry Hurwitz Health Assessment: Drs. Michael Antoni, Mary Catherine Segota, Jackie Junco Professional links: IACFS/ME on line: www.iacfs.net CDC on line: www.cdc.gov NIH on line: www.nih.gov