Download
1 / 49
490 likes | 624 Views
Acute Heart Failure Chief Rounds, Sept. 14, 2009 Dr. Frederic L. Ginsberg. CJTMEustaquio, MD PGY-3. Internal Medicine Cooper University Hospital. I. Introduction - Definition & Causes - General Approach II. Case 1: LS, 62M. cc: chest pain - Discussion: Management

E N D
Acute Heart FailureChief Rounds, Sept. 14, 2009Dr. Frederic L. Ginsberg CJTMEustaquio, MD PGY-3. Internal Medicine Cooper University Hospital
I. Introduction - Definition & Causes - General Approach II. Case 1: LS, 62M. cc: chest pain - Discussion: Management III. Case 2: DF, 60M. cc: syncope - Discussion: Management IV. Case 3: DK, 63F. cc: dyspnea - Discussion: Management V. Conclusion
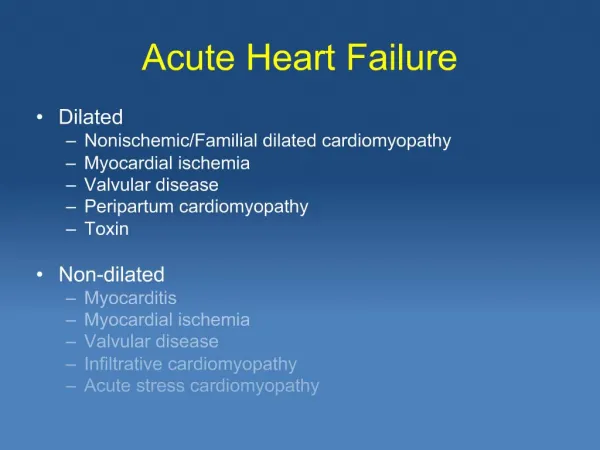
I. INTRODUCTION • Potentially fatal • Key concepts • Determinants of cardiac output • Heart failure - dyspnea • Introduction • Case 1 • Case 2 • Case 3 • Conclusion "demand >> supply"
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Congestive Heart Failure "volume of blood >> heart's capacity" no congestion congestion
Introduction • Case 1 • Case 2 • Case 3 • Conclusion • Acute decompensated heart failure - Potentially fatal • Cardiogenic pulmonary edema • Flash pulmonary edema
General Approach • Suspect the diagnosis from S/Sx - HPI: cough, SOB, fatigue, chest pain/ discomfort - PE: RR, HR, or BP accessory muscles wheezing S3, S4 gallop murmurs JVP pedal edema • Introduction • Case 1 • Case 2 • Case 3 • Conclusion
Consider precipitating factors CARDIAC MI & myocardial ischemia Atrial fibrillation, other arrhythmias Progression of underlying cardiac dysfunction RV pacing with dyssynchrony NON CARDIAC Severe HTN Renal failure Miscellaneous: anemia hypo/hyperthyroidism toxins (cocaine, EtOH) fever & infection uncontrolled DM Medications PE Dietary indiscretion, medication noncompliance, iatrogenic volume overload • Introduction • Case 1 • Case 2 • Case 3 • Conclusion
Introduction • Case 1 • Case 2 • Case 3 • Conclusion • Tests a. EKG b. CXR c. Lab data - CBC, basic chem 7, cardiac enzymes BNP, NT-proBNP Lipid profile, LFTs, TSH d. Echo e. Swan-Ganz catheter f. Coronary Angiography g. Others: EP studies • Treat
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 1: LS, 62M. Cc: chest pain • SSCP at rest SOB, dyspnea on exertion Diaphoresis • HTN, DM, HPL CAD s/p POBA 1991 Previous smoker • Metoprolol, HCTZ, Glyburide, Enalapril, Fish Oil, Lovastatin • 95.2F, 78, 164/83, 18, 99%RA No JVD. CTA b/l. RRR, good S1/S2, no m/r/g No pedal edema.
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Recommendations for the Evaluation of Patients with HF
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 1: LS, 62M. Cc: chest pain
Introduction • Case 1 • Case 2 • Case 3 • Conclusion • Diagnoses: • NSTEMI • Chronic Systolic Heart Failure 2 to severe CAD, • not in acute decompensation • HTN, DM, HPL
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Recommendations for the Evaluation of Patients with HF
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Recommendations for the Evaluation of Patients with HF
Introduction • Case 1 • Case 2 • Case 3 • Conclusion The Stages of Heart Failure – NYHA Classification
Introduction • Case 1 • Case 2 • Case 3 • Conclusion • Management: Medical + Evaluation for CABG - Thallium viability study: viable myocardium except distal apex - Discharged, then readmitted in 2 weeks for planned CABG x5: LIMA to D2 and LAD. SVG to D1. SVG to posterior descending artery & distal RCA.
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Treatment Recommendations for Patients at High Risk of Developing Heart Failure (Stage A)
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Treatment Recommendations for Patients with Asymptomatic LV Systolic Dysfunction (Stage B)
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Treatment Recommendations for Symptomatic LV Systolic Dysfunction (Stage C)
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Treatment Recommendations for Symptomatic LV Systolic Dysfunction (Stage C)
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 2: DF, 60M. Cc: Syncope
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 2: DF, 60M. Cc: Syncope • OSH: light headedness & syncope - (+) troponin - atrial flutter - severe hypotension – on Norepinephrine drip (Levophed) - transferred to CUH for cardiac catheterization • PMH: - Hepatitis C - s/p cholecystectomy - ESRD on HD - s/p patial colectomy 2 to polyps - NHL s/p chemo 2007 - s/p hernia repair - HTN - s/p AV fistula - ascites
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 2: DF, 60M. Cc: Syncope • SH: current smoker – 43py occasional EtOH former IVDA, quit 1978 • PE: afebrile, 127/91, HR=98, RR=30 • JVP=15 cm H20, 2+ carotid upstrokes • CTA B/L • RR, tachycardic, normal S1/S2 • Hepatomegaly • No LE edema
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 2: DF, 60M. Cc: Syncope
Diagnoses: - Acute Decompensated Heart Failure - Syncope. - NICMP EF 10-15%. - Paroxysmal atrial flutter. - ESRD. • Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 2: DF, 60M. Cc: Syncope
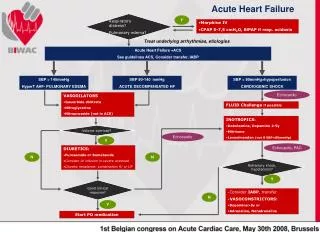
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Recommendations for the Management of Acute Heart Failure • Hospitalization • Hypotension, worsening renal function or altered mentation • Dyspnea at rest • Arrhythmia • ACS • In-patient monitoring • Hemodynamic monitoring • Treatment goals
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Goals of Initial Management of ADHF • Hemodynamic stabilization • Support of oxygenation and ventilation • Symptom relief
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Treatment Goals for Patients with ADHF • Improve symptoms • Optimize volume status • Identify etiology • Identify precipitating factors • Optimize chronic oral therapy • Minimize side effects • Identify patients who might benefit from revascularization • Educate
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Components of Therapy for ADHF • Na and fluid restriction • Diuretics • Oxygen and assisted ventilation • Morphine • Vasodilator – nitrate, nesiritide • Inotropic agents – dobutamine, milrinone • ACE inhibitors and ARBs • Beta-blockers
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 2: DF, 60M. Cc: Syncope • Medications: - ASA 325 mg daily - ISMN ER 30 mg daily - Carvedilol 25 mg BID - Hydralazine 10 mg TID - Valsartan 80 mg daily - Temazepam 30 mg daily - Gabapentin 300 mg BID - Percocet prn - Warfarin 2.5 mg daily
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Additional Considerations in ADHF • Arrhythmia management • Mechanical cardiac assistance • Ultrafiltration • Vasopressin receptor antagonist
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 2: DF, 60M. Cc: Syncope • EP studies, re atrial flutter. • TEE: no A-V clot • Atrial flutter ablation & ICD placement • Anticoagulation with Warfarin.
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 2: DF, 60M. Cc: Syncope Why the decision for an ICD during this admission vs. waiting 3 months of max medical therapy as in Case 1?
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Recommendations for Management of Concomitant Diseases in Patients with HF
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 2: DF, 60M. Cc: Syncope What inotropes are recommended had he still been hypotensive on transfer to CUH?
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 3: DK, 63F. Cc: dyspnea
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 3: DK, 63F. Cc: dyspnea • Admitted under GYN in May & June 2009, cc: Nausea, vomiting • Recent ovarian CA recurrence • Developed acute, severe SOB at rest while on the floors ICU transfer & BIPAP • PMH: - Ovarian CA 1997, s/p resection 1st recurrence, 2002. s/p chemo 2nd recurrence, May 2009. - HTN – Tenormin 80 mg daily - DM II – Metformin 500 mg BID, Pioglitazone 45mg daily - sulfa allergy
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 3: DK, 63F. Cc: dyspnea • FH: MI – father 75, brother 63 COPD – mother 64, sister • SH: no smoking, no EtOH • ROS: occasional palpitations, fatigue • PE: BP 124/55, HR 98 no JVD LLL crackles normal S1/S2, no murmurs, (+) S3 gallop no pedal edema
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 3: DK, 63F. Cc: dyspnea
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 3: DK, 63F. Cc: dyspnea • Diagnoses: - Acute decompensated heart failure (with cardiogenic pulmonary edema) - Cardiomyopathy with severe LV dysfunction, unclear etiology - Single vessel CAD – likely not the cause of CMP - DM II - HTN - Ovarian CA - HPL
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 3: DK, 63F. Cc: dyspnea • Medical therapy for ADHF • (IV Furosemide, Carvedilol, Lisinopril , ASA, statin. NPPV) symptomatic improvement back to GYN floors, discharged after 15 days • HF meds discontinued on D/C – unclear reason • Out-patient cardiology F/U within 1 week: - SOB much improved, only mild SOB on climbing 1 flight of stairs - back on Tenormin; not on beta blocker, ASA, ACE-I - Add ASA, Carvedilol. - Repeat echo in 2 weeks. - F/U with GYN re Tx plan for ovarian CA recurrence.
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Case 3: DK, 63F. Cc: dyspnea Takotsubo cardiomyopathy??
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Takotsubo cardiomyopathy • Stress-induced CMP • Apical ballooning syndrome • Broken heart syndrome • Transient LV systolic dysfunction • Mimics MI • No significant CAD
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Takotsubo Cardiomyopathy • Stress-induced • Acute medical illness / intense emotional stress / physical stress • Pathogenesis unknown • Catecholamine excess, coronary artery spasm, microvascular dysfunction
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Takotsubo Cardiomyopathy • Treatment and prognosis • Supportive • Hydration • Standard HF meds • ACE inhibitor • Beta-blocker • Diuretic • Aspirin • MR 0 – 8 % • Recovery in 1 to 4 weeks
Introduction • Case 1 • Case 2 • Case 3 • Conclusion Conclusion • Heart failure and ACS • ADHF in atrial flutter & ESRD • Takotsubo CMP • Evaluation guidelines in HF • Management principles in ADHF • Management of HF in general