Download
1 / 1
30 likes | 327 Views
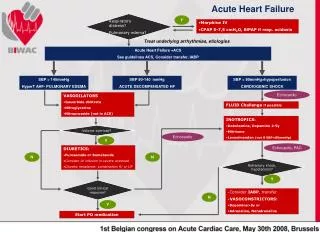
Respiratory distress? Pulmonary edema?. Acute Heart Failure. Y. Morphine IV CPAP 5-7,5 cmH 2 O, BiPAP if resp. acidosis. Treat underlying arrhythmias, etiologies. Acute Heart Failure +ACS See guidelines ACS, Consider transfer, IABP. SBP > 140mmHg HyperT AHF- PULMONARY EDEMA.

E N D
Respiratory distress? Pulmonary edema? Acute Heart Failure Y • Morphine IV • CPAP 5-7,5 cmH2O, BiPAP if resp. acidosis Treat underlying arrhythmias, etiologies Acute Heart Failure +ACS See guidelines ACS, Consider transfer, IABP SBP > 140mmHg HyperT AHF- PULMONARY EDEMA SBP 90-140 mmHg ACUTE DECOMPENSATED HF SBP < 90mmHg+hypoperfusion CARDIOGENIC SHOCK Echocardio • VASODILATORS • Isosorbide dinitrate • Nitroglycerine • Nitroprusside (not in ACS) FLUID Challenge if possible • INOTROPICS: • Dobutamine, Dopamine 2-5γ • Milrinone • Levosimendan (not if SBP<85mmHg) Volume overload? Echocardio Y Echocardio, PAC • DIURETICS: • Furosemide or Bumetanide • Consider IV infusion in severe overload • Diuretic resistance: combination R/ or UF N N Refractory shock, hypotension? Y Good clinicalresponse? • -Consider IABP, transfer • -VASOCONSTRICTORS: • Dopamine>5γor • Adrenaline, Noradrenaline N Y Start PO medication