Download
1 / 68
720 likes | 917 Views
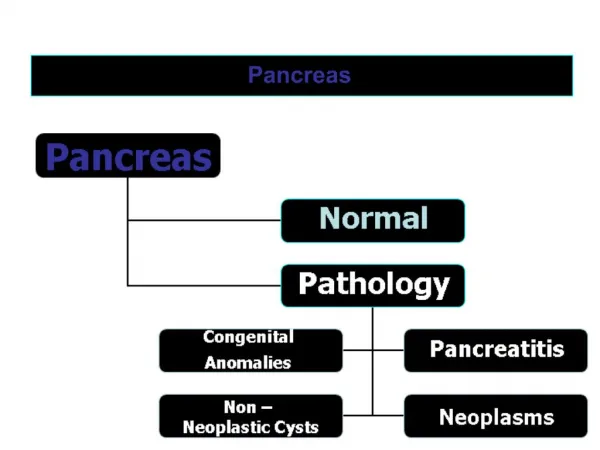
Pancreas. Acute pancreatitis. The term pancreatitis implies the presence of pancreatic inflammation and autodigestion It is classified into Acute (reversible no residue) form, which is either Acute pancreatitis Recurrent acute pancreatitis

E N D
Acute pancreatitis • The term pancreatitis implies the presence of pancreatic inflammation and autodigestion • It is classified into • Acute (reversible no residue) form, which is either • Acute pancreatitis • Recurrent acute pancreatitis • Chronic (progressive damage) form, which is either • Chronic pancreatitis • Chronic relapsing pancreatitis
Acute pancreatitis Pathogenesis • Common channel (biliary) • Pan-obstruction &hyper-secretion (Alcohol) • Back diffusion • Duodenal reflux
Acute pancreatitis • acute attack may ~>chronic pancreatitis if residual damage is left behind) • Each acute attack is classified as • Edematous (completely reversible) • Persistent (subsequent development of complications) • Hemorrhagic (fatal)
Acute pancreatitis (Etiology) • Idiopathic • Obstruction • Choledocolithiasis • Ampullary or pancreatic tumors • Pancreatic structural anomalies • Toxins • Alcohol • Drugs - salicylates, azathioprine, cimetidine • Trauma • Accidental • Iatrogenic • Metabolic abnormalities (hypercalcemia) • Infection • Vascular anomalies
Acute pancreatitis (Etiology) From the practical point of view the two conditions most commonly associated with acute pancreatitis are • Alcoholism (recurrent disease, the first attack is usually very severe getting less severe with recurrence and merging into chronic pancreatitis) • Biliary tract stone disease (older than 60, tends to be severe, frequently accompanied with complications and recurrence is preventable).
Clinical picture (Symptoms) The cardinal symptom of acute pancreatitis is abdominal pain, • Most often, it is located in the upper abdomen, usually epigastric, but may be perceived more on the left or right side, depending on which portion of the pancreas is involved. • which characteristically is dull, boring, and • steady in quality. • The pain radiates to the back in approximately one half of the cases. • Associated symptoms such as anorexia, nausea, and vomiting are common, and some patients experience diarrhea
Clinical picture (Sings) • The findings on physical examination that follow are variable, depending on the severity of the disease. • General • Pulse------ Tachycardia are common abnormal vital sign. • Temp----- Fever are common abnormal vital sign. • Respiratory rate--- Few patients experience dyspnea (10%), which may be caused by irritation of the diaphragm, resulting from inflammation, or a more serious condition, such as respiratory distress syndrome. • BP------In severe cases, hemodynamic instability is evident (10%), • A minority of patients exhibits jaundice • Profound shock and cyanosis
Clinical picture (Sings) • Local • Abdominal tenderness, muscular guarding, and distension are observed in most patients. Bowel sounds often are hypoactive. • Sometimes, hematemesis or melena develops (5%).
Clinical picture (Sings) • A few local uncommon physical findings are associated with severe necrotizing pancreatitis. • The Cullen sign is a bluish discoloration around the umbilicus, resulting from hemoperitoneum. • The Grey-Turner sign is a reddish-brown discoloration along the flanks, resulting from retroperitoneal blood dissecting along tissue planes. • Erythematous skin nodules may result from focal subcutaneous fat necrosis
Diagnostic procedures Nonspecific investigations • CBC • increased hematocrit due to hemoconcentration • Leucocytosis • X ray chest • elevation of copulae, • basal atalectasis, • left sided or bilateral effusions • ECG will show transient signs of ischemia
Diagnostic procedures Laboratory investigations • Serum amylase (elevated for 3 days mainly) • Attain 5 times the normal or more • If persistently elevated >10 days it means complication • Other diseases can give elevations (acute cholecystitis, and perforated DU) • Urine amylase • Serum lipase • Serum bilirubin • Hyperglycemia and glucosuria • Hypocalcemia (can cause tetany, is due to saponification of omentum) • CBC Leucocytosis and anaemia • Immunoreactive trypsin and elastase
Diagnostic procedures Radiological investigations • Plain abdomen, standing • Sentinel jujenal loop, or paralytic ileus • Granular calcification of chronic pancratitis • Radio-opaque gall stones • Colon cut off sign • Abdominal ultrasound • This is the most useful initial test in determining the etiology of pancreatitis and is the technique of choice for detecting gallstones. • In the setting of acute pancreatitis, sensitivity is reduced to 70-80%. • CT scan
Contrast-enhanced CT scoring system • A-----Normal • B-----Focal or diffuse glandular enlargement or small intra-pancreatic fluid collection • C-----Peripancreatic inflammatory changes or less than 25% gland necrosis (concentration of contrast dye) • D------Single extrapancreatic fluid collection, or 25-50% gland necrosis, or extensive extrapancreatic fluid collection. • E----Pancreatic abscess,or more than 50% gland necrosis
Other imaging techniques • Endoscopic ultrasonography • Endoscopic ultrasonography (EUS) is an endoscopic procedure that allows a high-frequency ultrasound transducer to be inserted into the gastrointestinal tract to visualize the pancreas and biliary tract. • Magnetic resonance cholangiopancreatography • (MRCP) has an emerging role in the diagnosis of suspected biliary and pancreatic duct obstruction in the setting of pancreatitis.
Differential diagnosis (DD) • Early 2 to 3 h acute cholecystitis • After 6 to 8 h perforated DU or acute appendicitis • After 2 to 3 days intestinal obstruction • If presentation is with profound shock the DD is myocardial infarction, aortic dissection, ruptured aortic aneurysm, or mesentric infarction
Natural history • 80% of patients have mild pancreatitis with good recovery • Mild disease accounts for less than 5% of the mortality from pancreatitis • Mortality from pancreatitis due to: • Early multiple organ failure • Late infected pancreatic necrosis • Hemorrhage • Associated co-morbidity • Aim of prognostic scores is to identify patients with severe pancreatitis
Bad prognostic markers (Ranson) • On admission AGLS • Age>55 • Fasting blood gulcose >200mg% • Leucocytosis (WBC >16,000) • LDH in serum >350 iu/L • SGOT>250 units%
Bad prognostic markers (Ranson) initial 48 hours of admission HAF CUP • Hematocrit decrease >10% • Acidosis (base deficit >4 m Eq/L) • Estimated Fluid sequestration > 6 liters • Serum calcium<8mg • BUN increase > 5 mg% • PO2 Arterial tension < 60mmHg
Bad prognostic markers (Ranson) • > 3~> mortality < 1% • 3-4~> mortality 18%, • 5-6~> mortality 50%, • >6~> mortality 90%
Medical treatment (Acute management): • Treat shock. Invasive hemodynamic monitoring may be required. May need up to 6-8 liters of fluid per day. • An NG tube useful for those with vomiting. However, NG tubes have not been shown to reduce the duration of hospitalization nor do they decrease pain intensity associated with pancreatitis. • Keep the patient NPO until pain resolves and analgesia is no longer required. • NPO for 7 days in mild and • 14 days in severe is a must. • TPN can be used as a nutritional support.
Medical treatment (Acute management): • Prevent hypocalcemia and hypomagnesemia. • Manage pain with parenteral patient-controlled narcotics. Meperidine is preferred in the case of a common duct stone. Morphine is otherwise a good choice. (Adequate analgesia - opiate or epidural) • Keep stomach pH close to neutral by using prentral proton pump inhibitors. • Octreotide has not been shown to be useful in treating pancreatitis. However Lexipafant – A platelet activating factor antagonist can be useful
Medical treatment (Acute management): • Urgent ERCP to clear the biliary tract has been shown to reduce morbidity and mortality in severe acute biliary pancreatitis. • Antibiotics (for the associated ascending cholangitis) are indicated. • In several trials, imipenemhas been shown to have good penetration into pancreatic tissue, and it has a good activity against all likely pathogens. • Other antibiotics that have been shown to be efficacious in acute necrotizing pancreatitis include cefuroxime and a regimen of ceftazidime, amikacin, and metronidazole.
Medical treatment (Acute management): • Close monitoring of • Hemocynamics • blood gases • local condition by repeated CT or less efficiently U/S and • treat organ failure as indicated. e.g. • dialysis in renal failure • oxygen therapy and PEEP in ADRS etc.
Early surgeryIndications • When the diagnosis is in doubt • Failure of the patient to improve on medical treatment. • Patients with known biliary stone disease with no improvement within 48 to 72 hours • For patients who improve, they should undergo operation for cholelithiasis as soon as the pancreatitis subsides (preferably during same hospitalization)
Surgical procedures in early intervention • Inspection only • Placement of catheters for peritoneal lavage • Biliary decompression via cholecystostomy or T tube in CBD • Cholecystectomy, CBD exploration for stone extraction • Decompressing gastrostomy and feeding jujenostomy • For pancreatic abscess or extensive necrosis • Total or subtotal pancreatic necrosectomy • Pancreatic and retroperitoneal debridement and drainage
Complications of acute pancreatitis Local • Necrosis +/- infection(pancreatic abscess) • Pancreatic fluid collections (pseudocyst of the pancreas) • Colonic necrosis • Gastrointestinal hemorrhage • Splenic rupture
Complications of acute pancreatitis Systemic • Hypovolaemia and shock • Coagulopathy • Respiratory failure • Renal Failure • Hyperglycaemia • Hypocalcaemia
Complications of acute pancreatitis Pseudocyst formation • Is a collection of fluid, serum and hematoma in the lesser sac with a connection at some point with glandular tissue or ductal system? Abscess formation (usually after second week) • It implies the presence of extensive pancreatic and peripancreatic necrosis with secondary infection (not merely infected pseudocyst) Hemorrhage • From pseudoaneurysm of splenic artery or left sided portal hypertension due to splenic V thrombosis
Pseudocyst Surgery depends on five items • Size (<5 cm is likely to resolve, while >7.5 will need drainage) • Development of symptoms (will indicate complications, rupture, infection or hemorrhage) • Maturity (4 to 6 weeks for acute cysts to mature for better internal drainage) • Vascular complications associated with pseudocyst (pseudoaneurysm is an indication for resection rather than drainage, and left sided portal hypertension is an indication of splenectomy) • Site • retrogastric ~>cystogastrostomy, • head ~>cystoduodenostomy, and • inferior~>cystojujenostomy by Roux en Y)
Pseudocyst • Internal drainage (cyst-enterostomy) is the rule. • External drainage • Infected or ruptured or acute cysts~> drain externally usingsump drain the resulting pancreatic fistula will spontaneously close • CT or U/S guided external drainage has special indications where the patient cannot tolerate surgery in infected or acute cysts with rapid enlargement
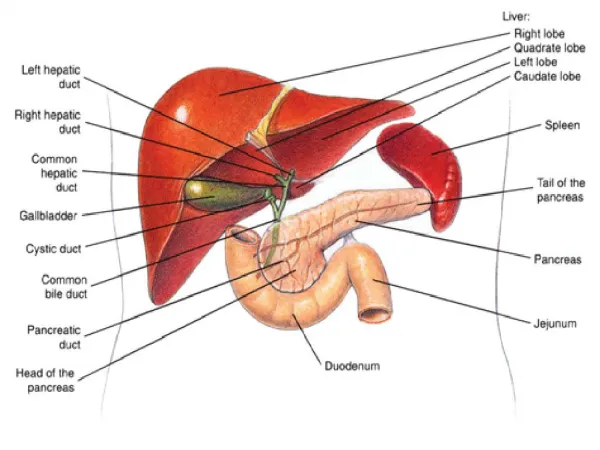
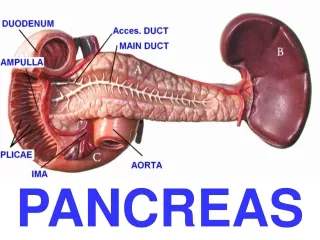
Cancer Pancreas • In clinical practice, pancreatic cancer is synonymous with pancreatic ductal adenocarcinoma, which constitutes 90% of all primary malignant tumors arising from the gland. • When cancer originates in the head of the pancreas (70%) • it must also be differentiated from cancer originating from the ampulla, duodenum or lower common bile duct which has a much better prognosis than true pancreatic cancer
Risk factors • Diabetes • Chronic pancreatitis, and alcoholism • Tobacco, coffee • Previous radiation • Genetics. Approximately 5-10% of patients with pancreatic carcinoma have some genetic predisposition to developing the disease.
Clinical picture Cancer head Symptoms • Triad of • jaundice (progressive and deep) with • pain and • loss of weight with anorexia is extremely common • Vomiting, change in bowel habit and hematemesis and or melena occurs if the tumor invades or compresses the duodenum Signs • General----Chills and fever and toxemia is due ascending cholangitis • Local • Palpable GB (Courvoisier’s sign), • palpable liver (hydrohepatosis) are important signs
Clinical picture Cancer body and tail Symptoms • Pain and weight loss are the two main symptoms. • Pain is girdle like or in epigastrium with posterior radiation, with patient leaning forward, it may be related to meals • Hematemesis, may be due to left sided portal hypertension Signs • Trouseau’s signs, migrating thrombophlebitis • Troisier’s signs (Virschow’s LN) • Abdominal masses or malignant liver, ascites, Blummer shelf or
Coourvoisier”s law Coourvoisier”s law states that, • if in a jaundiced patient, the gall bladder is enlarged, • it is not a case of a stone impacted in the CBD for previous cholycystitis • which existed when the stone was in the gall bladder, • must have rendered the gall bladder fibrotic and incapable of dilatation.
Coourvoisier”s law Exceptions are • Double stones, one in the CBD and another in the cystic duct, the later will force the gall bladder to distend • Klatskin tumor, with carinal obstructin leaving the gal bladder not distended • Ampullary tumor with no complete obstruction with intermittent relief of jaundice will not enforce the gall bladder to enlarge • A gall bladder situated beneath the liver in an obese patient and cannot be palpated is another exception
Investigations • Liver function • Glucose tolerance curve • Tumor markers • Carcinoembryonic antigen (CEA) • It is a high molecular weight glycoprotein found normally in fetal tissues. • The reference range is less than or equal to 2.5 mg/mL. • Only 40-45% of patients with pancreatic carcinoma have elevations in CEA levels. • Another tumor marker is carbohydrate antigen 19-9 (CA 19-9 )
Investigations • Doppler ultrasound allows assessment of vascular invasion. Mesenteric angiography is now considered obsolete replaced by Doppler ultrasound • CT completes the U/S especially as regards the pancreatic tumors • Endoscopic ultrasound • EUS has detection rates of 99-100% for all pancreatic carcinomas, including those smaller than 3 cm. EUS is as accurate as ERCP or MRCP for assessing the etiology of obstructive jaundice.
Investigations • Endoscopic retrograde cholangiopancreatography • ERCP is highly sensitive for helping detect pancreatic carcinoma. Of patients with pancreatic adenocarcinoma, 90-95% have abnormalities on ERCP findings. • More recently, brush cytology and forceps biopsy at the time of ERCP have been used to histologically diagnose pancreatic carcinoma; • ERCP does have the advantage of allowing for therapeutic palliation of obstructive jaundice with either a plastic or metal biliary stent.
Investigations • Laparoscopy • Laparoscopy will identify liver or peritoneal metastases in 25% of patients deemed resectable after conventional imaging. • Laparoscopic ultrasound has improved predictability of resection.
Staging of pancreatic tumors is as follows: • Tumor (T) • TX - Primary tumor cannot be assessed • T0 - No evidence of primary tumor • Tis - Carcinoma in situ • T1 - Tumor limited to the pancreas, 2 cm or smaller in greatest dimension • T2 - Tumor limited to the pancreas, larger than 2 cm in greatest dimension • T3 - Tumor extension directly into duodenum, bile duct, or peripancreatic tissues • T4 - Tumor extension directly into stomach, spleen, colon, or adjacent large vessels