TUBULAR REABSORPTION
250 likes | 626 Views
TUBULAR REABSORPTION. URINARY BLOCK 313. Dr. Shaikh Mujeeb Ahmed Assistant Professor AlMaarefa College. Objectives. Define tubular secretion Role of tubular secretion in maintaining K + conc. Mechanisms of tubular secretion. URINE FORMATION.

TUBULAR REABSORPTION
E N D
Presentation Transcript
TUBULAR REABSORPTION URINARY BLOCK 313 Dr. ShaikhMujeeb Ahmed Assistant Professor AlMaarefa College
Objectives • Define tubular secretion • Role of tubular secretion in maintaining K+ conc. • Mechanisms of tubular secretion.
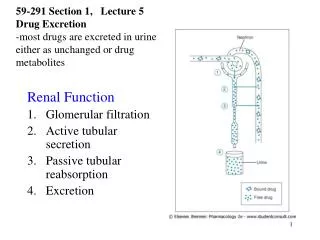
URINE FORMATION • Three Basic Mechanisms (Renal Processes) Of Urine Formation include: • Glomerular Filtration • Tubular Reabsorption • Tubular Secretion
Tubular secretion • Secretion – transfer of material from blood into tubular fluid • Helps control blood pH • Helps eliminate substances from the body
Tubular Secretion • First step is simple diffusion from peritubular • capillaries to interstitial fluid • Enter to tubular cell can be active or passive • Exit from tubular cell to lumen can be active or • passive • Examples:potassium, hydrogen, organic acids, • organic bases, NH3
Calculation of Tubular Secretion Secretion = Excretion - Filtration H+, K+,NH3 Organic acids and bases
Tubular Secretion • Tubular secretion is important for: • Disposing of substances not already in the filtrate • Eliminating undesirable substances such as urea and uric acid • Ridding the body of excess potassium ions • Controlling blood pH by secreting H+
Tubular Secretion • Most important substances secreted by the tubules: • H+ • Important in regulating acid-base balance • Secreted in proximal, distal, and collecting tubules • K+ • Keeps plasma K+ concentration at appropriate level to maintain normal membrane excitability in muscles and nerves • Secreted only in the distal and collecting tubules under control of aldosterone • Organic ions • Accomplish more efficient elimination of foreign organic compounds from the body • Secreted only in the proximal tubule
Potassium balance • 98% of K+ is in ICF & 2% in ECF • ICF = 150 m Eq/L & in ECF = 4.5 mEq/L • Balance → intake = out put • Maintenance of K balance is important in normal functioning of excitable tissue
Importance of regulating plasma K+ concentration • K+ plays a key role in the membrane potential of excitable tissues. • Both increase and decrease in plasma K+ can change intracellular to extracellular K+ conc. Gradient which can change the RMP. • Its impact on the heart – decreased cardiac excitability • Rise in ECF K+ conc. decreases excitability of the neurons & skeletal muscle cells. • Decrease in ECF K+ lead to skeletal muscle weakness, diarrhea and abdominal distension.
Potassium handling by nephron(continued) • Distal tubule & collecting ducts : • Responsible for adjustment ofK+excretion by either re absorption or secretion as dictated by need • α -Intercalated cells : absorption of potassium if person is on low K+ diet • Principle cells : if person on normal or high K+ diet potassium is excreted by principle cells • The magnitude of potassium excretion is variable depending on diet & several other factors for eg.aldosterone,acid base status ,flow rate etc
Effect of H+ secretion on K+ secretion During acidosis H+ secretion is increase lead to retention of K+.
Factors affecting K+secretion • Magnitude of K+ secretion is determined by the size of electrochemical gradient across luminal membrane • Diet: High K+ diet concentration inside thus principle cells increases electrochemical gradient across membrane
Factors affecting K+secretion(continued) • Aldosterone : • Aldosterone Na+ re absorption by principle cell by inducing synthesis of luminal membrane Na+ channels & basolateral membrane Na+- K+ channel • more Na+ is pumped out of the cell simultaneously more K+ pumped into the cell • Thus increasing the electrochemical gradient for K+ across the luminal membrane that leads to increase K+ secretion
DUAL EFFECT OF ALDOSTERONE Fall in Na+ - through RAAS Increase in K+
Late Distal, Cortical and Medullary Collecting Tubules Tubular Lumen Principal Cells H20 (+ ADH) Na + Na + ATP ATP K+ K+ Cl- Aldosterone
Aldosterone Actions on Late Distal, Cortical and Medullary Collecting Tubules • Increases Na+ reabsorption -principal cells • Increases K+ secretion - principal cells • Increases H+ secretion - intercalated cells
Relationship between Na+ absorption & K+ secretion • High Na+ diet: • more Na+ will be delivered to principle cells ,more Na+ is available for Na+- K+ATPase than more K+ is pumped into the cell which increases the driving force for K+ secretion • Diuretics : • loop & thiazide diuretics inhibit Na+ re absorption in part of tubule earlier to principle cells, so increases Na+ delivery to principle cells , more Na+ is reabsorbed & more K+ is excreted
Organic Anion and Cation secretion • Proximal tubule contains two types of secretory carriers • For organic anions • For organic cations • Organic ions such as Prostaglandin, epinephrine – after their action removed from blood • Non filterable organic ions also removed • Chemicals, food additives, non nutritive substances • Drugs – NSAID, antibiotics
PAH –EXAMPLE OF SECRETION • PAH is an organic acid • Used for measurement of renal plasma flow • Both filtered and secreted • PAH transporters located in peritubular membrane of proximal tubular cells. • There are parallel secretory mechanism for secretion of organic bases like quinine and morphine
UREA & Uric acid • Urea is freely filtered – 50% reabsorbed in PCT. • Urate is freely filtered • In PCT there is reabsorption and secretion takes place. • In the initial & middle part of PCT reapsorption is more than secretion • In the distal portion of PCT moderate amount of urates are secreted.
References • Human physiology by Lauralee Sherwood, seventh edition • Text book of physiology by Linda .s contanzo,third edition • Text book physiology by Guyton &Hall,11th edition