Download
1 / 21
210 likes | 531 Views
Learn about sinonasal malignancies, their epidemiology, etiology, and pathophysiology. Understand symptoms and diagnostic workup including imaging studies like MRI and CT scans.

E N D
Sinus Cancer Reporter: clerk 柯仁裕Supervisor: 戴志峰 醫師
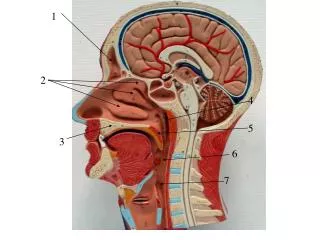
Background • The location of the nasal cavity and the paranasal sinuses make them extremely close to vital structures. • Sinonasal malignancies (SNM) can grow to considerable size before presentation, and aggressive therapy may be needed in areas close to the skull base, orbits, cranial nerves, and vital blood vessels
Sinonasal malignancies (SNM)---the initial manifestations (eg, unilateral epistaxis, nasal obstruction) mimic signs and symptoms of many common but less serious conditions. • The patient and clinician often ignore or minimize the initial presentation of these tumors and treat early-stage malignancy as a benign sinonasal disorder. • By the time ominous signs and symptoms (such as severe intractable headache, visual disturbance, or cranial neuropathy) occur, the neoplasm is often advanced.
Epidemiology • Sinonasal malignancies (SNM) are rare. They are more common in Asia and Africa than in the United States. • In parts of Asia, sinonasal malignancies (SNM) are the second most common head and neck cancer behind nasopharyngeal carcinoma. Men are affected 1.5 times more often than women, and 80% of these tumors occur in people aged 45-85 years. • Approximately 60-70% maxillary sinus 20-30% nasal cavity 10-15% ethmoid air cells (sinuses) the remaining frontal & sphenoid sinuses
Etiology • Risk factors for sinonasal malignancies (SNM) are complicated, multifactorial, and somewhat controversial. • Squamous cell carcinoma (SCC) and adenocarcinoma in this area are associated with exposure to nickel dust, mustard gas(dichlorodiethyl sulfide), thorotrast(二氧化釷,放射性顯影劑), isopropyl oil, chromium(鉻) is well established. • Wood dust exposure, in particular, is found to increase the risk of SCC 21 times and the risk of adenocarcinoma 874 times. • Many of these products are found in the furniture-making industry, the leather industry, and the textile industry.
Pathophysiology • Squamous cell carcinoma (SCC) 80% of all malignancies that arise in the nasal cavity and paranasal sinuses. Approximately 70% occurs in the maxillary sinus, 12% in the nasal cavity, and the remainder in the nasal vestibule and remaining sinuses.
Adenoid cystic carcinoma (ACC) salivary origin and is the second most common sinonasal malignancy, accounting for 10% of cases. • Three histological subtypes are based on growth patters: tubular, cribriform, and solid. The solid form portends a much worse prognosis than either cribriform or tubular.
Adenocarcinoma associated with specific risk factors including exposure to wood dust, lacquers(亮光漆), and other organic compounds. • Distant metastases are rare. When they do occur, the lung, liver, and bone are the sites most often involved. Metastases to the cervical lymph nodes are uncommon, even with poorly differentiated tumors.
Malignant melanoma • Sinonasal neuroendocrine tumors • Esthesioneuroblastoma (ENB, olfactory neuroblastoma) • Sinonasal undifferentiated carcinoma (SNUC) • Small cell neuroendocrine carcinoma (SmCC) • Lymphoma • Salivary-type neoplasms • Sarcoma • Metastatic tumors
Presentation • Initial presenting symptoms include epistaxis, nasal obstruction, recurrent sinusitis, cranial neuropathy, sinus pain, facial paresthesia, proptosis, diplopia, or an asymptomatic neck mass. • Often, these mimic signs of conditions more common and less serious than malignant tumors of the sinuses. The patient often ignores early symptoms, or the clinician may minimize them, treating early-stage malignancies as infectious diseases.
The ominous signs and symptoms (eg, severe intractable headache, visual disturbances) occur, the neoplasms are advanced and require complex management.
Workup • Laboratory Studies • As with other head and neck cancers, liver enzymes are usually obtained to assess for distant disease in addition to a chest radiograph or CT scan to evaluate for pulmonary metastasis • In the case of a nasal cavity or paranasal sinus mass or erosion, an antineutrophil cytoplasmic antibody (ANCA) test for possible Wegener granulomatosis should be considered. This condition often mimics a neoplasm.
Imaging Studies • Magnetic resonance imaging (MRI): determine resectability such as orbital invasion, perineural spread, skull base invasion, intracranial extension • One of MRI’s greatest uses is in helping to demonstrate the distinction tumor and retaining secretions in the multiple sinus cavities.
CT scan has a higher accuracy at determining both bony remodeling and erosion of the skull base and sinuses. • Osteolysis can often be observed with SCC, metastatic disease, sarcoma, and sinonasal undifferentiated carcinoma(SNUC). • Boney remodeling is more often seen with salivary gland tumors, large cell lymphoma, melanoma, and esthesioneuroblastoma(ENB). • CT scanning is slightly more accurate than MRI in demonstration of orbital invasion due to its ability to evaluate both the bony orbital wall and adjacent fat.
Diagnostic Procedures • Biopsy is the only 100% accurate means of obtaining a tissue diagnosis. • Remember that the turbinates and the possibility of a juvenile angiofibroma may both lead to extensive bleeding. • A biopsy should be performed on highly suspicious vascular tumors in the OR under controlled conditions where bleeding can be more safely controlled.
Staging • Staging of nasal cavity and paranasal sinus carcinomas is not as well established as for other head and neck tumors. • Two generally accepted staging systems are currently in use. The Kadish staging system is used specifically for Esthesioneuroblastoma because this often involves the skull base and intracranial extension. • For cancer of the maxillary sinus, the nasal cavity, and the ethmoid sinus, the American Joint Committee on Cancer (AJCC) has designated staging by TNM classification. • No broadly accepted staging systems for frontal and sphenoid sinus cancer currently exist
Maxillary sinus • Primary tumor (T) • T1 - Tumor limited to maxillary sinus mucosa with no erosion or destruction of bone • T2 - Tumor causing bone erosion or destruction including extension into the hard palate and/or the middle of the nasal meatus, except extension to the posterior wall of maxillary sinus and pterygoid plates • T3 - Tumor invades any of the following: bone of the posterior wall of maxillary sinus, subcutaneous tissues, floor or medial wall of orbit, pterygoid fossa, ethmoid sinuses • T4a - Tumor invades anterior orbital contents, skin of cheek, pterygoid plates, infratemporal fossa, cribriform plate, sphenoid or frontal sinuses • T4b - Tumor invades any of the following: orbital apex, dura, brain, middle cranial fossa, cranial nerves other than maxillary division of trigeminal nerve (V2), nasopharynx, or clivus
Nasal cavity and ethmoid sinus • Primary tumor (T) • T1 - Tumor restricted to any one subsite, with or without bony invasion • T2 - Tumor invading 2 subsites in a single region or extending to involve an adjacent region within the nasoethmoidal complex, with or without bony invasion • T3 - Tumor extends to invade the medial wall or floor of the orbit, maxillary sinus, palate, or cribriform plate • T4a - Tumor invades any of the following: anterior orbital contents, skin of nose or cheek, minimal extension to anterior cranial fossa, pterygoid plates, sphenoid or frontal sinuses • T4b - Tumor invades any of the following: orbital apex, dura, brain, middle cranial fossa, cranial nerves other than (V2), nasopharynx, or clivus
Regional lymph nodes (N) • N1 - Metastasis in a single ipsilateral lymph node, 3 cm or less in greatest dimension • N2a - Metastasis in a single ipsilateral lymph node more than 3 cm but 6 cm or less in greatest dimension • N2b - Metastasis in multiple ipsilateral lymph nodes, 6 cm or less in greatest dimension • N2c - Metastasis in bilateral or contralateral lymph nodes, 6 cm or less in greatest dimension • N3 - Metastasis in a lymph node more than 6 cm in greatest dimension
Kadish Staging for esthesioneuroblastoma • Stage A: The tumor is limited to the nasal fossa. • Stage B: The tumor extends to the paranasal sinuses. • Stage C: The tumor extends beyond the paranasal sinuses.