Download
1 / 1
20 likes | 157 Views
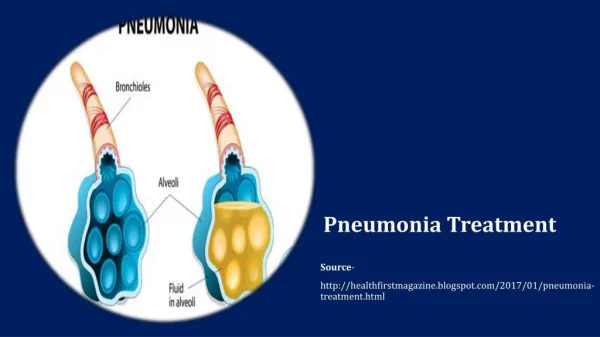
TREATMENT OF SEVERE PNEUMONIA WITH ORAL ANTIBIOTICS. Lozano JM , on behalf of the APPIS Trial Group . Department of Pediatrics and Clinical Epidemiology Unit, School of Medicine, Pontificia Universidad Javeriana, Bogotá, Colombia. Abstract TREATMENT OF SEVERE PNEUMONIA WITH ORAL ANTIBIOTICS

E N D
TREATMENT OF SEVERE PNEUMONIA WITH ORAL ANTIBIOTICS Lozano JM, on behalf of the APPIS Trial Group. Department of Pediatrics and Clinical Epidemiology Unit, School of Medicine, Pontificia Universidad Javeriana, Bogotá, Colombia Abstract TREATMENT OF SEVERE PNEUMONIA WITH ORAL ANTIBIOTICS Lozano JM, on behalf of the APPIS Trial Group. Javeriana University, Bogotá, Colombia Problem Statement: Injectable penicillin is recommended treatment for WHO-defined severe pneumonia. Oral amoxicillin, if found equally effective, could reduce referral, hospitalisation and treatment costs. Objectives: To determine whether an equivalent proportion of children aged 3-59 months with severe pneumonia improves after 48 hours of treatment with oral amoxicillin or injectable penicillin. Design: Open equivalence randomised trial. Setting: Nine tertiary care hospitals in eight countries. Study Population: 1,702 hospitalised children with clinically severe pneumonia (cough and/or difficult breathing plus chest indrawing). Intervention(s): IV benzyl penicillin (200.000 U/kg/day) or oral amoxicillin (45 mg/kg/day). Outcome Measure(s): Main: the proportion of children who failed to improve or worsened at 48 hours of treatment. Secondary: the proportion of failures or relapses at 5 and 14 days and of side effects. Results: 845 subjects were allocated to penicillin and 857 to amoxicillin. There was no significant difference in the proportion of failures at 48 hours (penicillin 161 [19%], amoxicillin 167 [19%]; rate difference -0.4%, 95% CI -4.2% to 3.3%). Cumulative treatment failures at 5 and 14 days were also equally distributed in the two groups. A total of 11 and 4 deaths were observed within 30 days in the penicillin and in the amoxicillin groups, respectively (difference 0.8%, 95% CI –0.1% to 2%). Infancy (OR 2.72, 95% CI 1.95 to 3.79), very fast breathing (1.94, 1.42 to 2.65) and hypoxia (1.95, 1.34 to 2.82) at baseline predicted treatment failure by multivariate analysis. Conclusions: Oral amoxicillin and parenteral penicillin are equally effective in the treatment of hospitalised children with severe pneumonia in developing countries. Funding Source(s): Department of Child and Adolescent Health and Development, World Health Organization; Applied Research in Child Health (ARCH) Project; USAID. Results • Introduction • Standard WHO guidelines recommend that children with severe pneumonia (acute respiratory infection (ARI) and lower chest wall indrawing (LCI)) be hospitalized and treated with parenteral antibiotics. However, hospitalization required for the administration of injectable therapy has several drawbacks: • It is associated with an increased risk of morbidity • in some settings injection needles and administration equipment are in short supply or periodically unavailable • hospitalization can substantially increase the cost of health care • referred children may not be brought or able to get to the hospital • Research Questions • Primary.Is treatment failure at 48 h among children aged 3-59 months with WHO-defined severe pneumonia treated with oral amoxicillin equivalent to that with injectable penicillin? • Secondary. Do the two treatments remain clinically equivalent through follow-up on days 5 and 14? • Discussion • Oral amoxicillin and injectable penicillin have equivalent clinical efficacy at 48 hours and beyond. • The relatively high failure rate for severe pneumonia can be partially explained by the rather stringent clinical criteria used to establish treatment failure at this endpoint. The low case fatality rate supports this observation. • RSV was identified in one quarter of the children, which is consistent with the median age of subjects in our study (8 months) . This is similar to previously reported data from developing countries. • An increased failure rate among HIV-infected children was observed in Durban and Ndola (data not shown). This suggests that empiric treatment of severe pneumonia with oral amoxicillin or parenteral penicillin alone may be insufficient in areas of high HIV prevalence. • Infancy, severe tachypnea and hypoxemia were predictive of treatment failure at 48 hours in a multivariable model (data not shown). These have also been reported elsewhere as predictors of therapy failure for pneumonia. Methods Design. Randomized non-blinded equivalency trial. Setting. Tertiary care facilities at 9 international sites: Colombia, Ghana, India, Mexico, Pakistan, South Africa (2 sites), Vietnam and Zambia. Study population. Children aged 3 to 59 months with WHO-defined severe pneumonia (lower chest indrawing in children with cough and/or difficult breathing) were eligible. Children with a recent history of very severe infectious/non infectious disease, chronic or congenital illness, asthma, clinically evident HIV infection, persistent vomiting, known penicillin allergy or more than 48 hours of antibiotic therapy for the present illness were excluded. Written informed consent was obtained from legal guardians. Randomization and Interventions. Randomization lists, stratified by site, were prepared in advance and implemented using sealed, opaque and numbered envelopes. Children were assigned to either oral amoxicillin syrup (45mg/kg/day divided in three doses) or parenteral penicillin G (200,000 IU/kg/day divided in four doses). Outcomes. All subjects were hospitalized for at least 48 hours. Children whose clinical status improved were discharged at 48 hours with a course of oral amoxicillin and asked to return for reassessments at 5 days and 14 days. Treatment failure up to or at 48 hours of randomization was defined as the appearance of danger signs, low oxygen saturation, persistence of LCI at 48 hours, life-threatening or serious adverse drug reaction, receiving another antibiotic, newly diagnosed co-morbid condition, parents/guardian withdrew consent, child left against medical advice or death • Conclusions • This study demonstrates clinical equivalency between injectable penicillin and oral amoxicillin in the treatment of severe pneumonia. These finding have several important beneficial implications: • reducing the risk of needle-associated complications and needle-borne infections • decrease treatment administration costs • the full public health benefit of these findings will depend on additional research which determines the role of oral amoxicillin in the treatment of severe pneumonia at the community or household level.