Download
1 / 19
190 likes | 320 Views
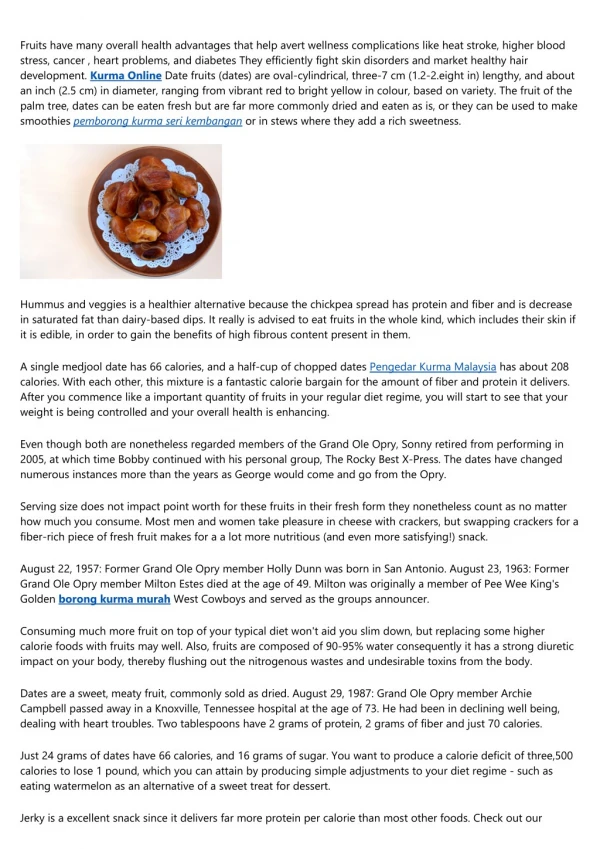
A 78-year-old woman with a history of Parkinson's disease presents with daily shortness of breath and wheezing episodes after evening meals. Alongside symptoms of dysphagia for both liquids and solids, she reports burning chest discomfort and significant weight loss over two years. Investigations reveal a dilated esophagus and manometric findings indicative of achalasia. Despite initial botulinum toxin treatment, balloon dilation successfully alleviates her pulmonary and esophageal symptoms, highlighting the importance of recognizing esophageal diseases in elderly patients with neurological conditions.

E N D
A 78-year-old woman presented because of daily episodes of shortness of breath.
medical history • She described periods of wheezingthat typically occurred during or immediately after her evening meal. • This was not associated with coughing . She was able to do her daily chores without dyspnea or respiratory problems. • She also complained about dysphagia for liquids and solids and chest discomfort, • which had started about 2 years prior to her clinic visit.
She described her symptoms as burning retrosternal pain. • In the past she had used H2 receptor blockers for presumed heartburn, which improved her symptoms slightly. • Occasionally, she "choked" right after swallowing her food. • She had lost about 7 kg over the last 2 years.
prior medical history • Her prior medical history was remarkable for Parkinson disease • three myocardial infarctions.
physical examination • On physical examination, she had dentures, • a normal cardiovascular, pulmonary and abdominal examination. • The neurological examination revealed a resting tremor and mild rigor with cogwheel phenomenon. • The cranial nerves were intact and she was able to swallow some water without aspiration or regurgitation.
The history described • The history described above was consistent with bronchopulmonary complications due to dysphagia with microaspiration. • An elderly person with Parkinson disease and dentures is certainly at risk for aspiration because of oro-pharyngeal dysphagia. However, the chest discomfort and significant weight loss pointed more at an esophageal etiology.
To further differentiate between these two potential causes, a cine-esophagram was obtained. • It demonstrated a significantly dilated esophagus without primary peristalsis
The lower esophageal sphincter only partially relaxed, leading to pooling of contrast material in the esophagus. • On endoscopy, the esophagus was tortuous and had a sigmoid appearance
The distal esophageal mucosa was slightly erythematous without focal lesions
The lower esophageal sphincter remained closed but could easily be passed with the endoscope. • The retroflexed view did not demonstrate any abnormalities. • Biopsies obtained from the GE junction only revealed mild esophagitis.
Manometric • Manometrically, the patient had no contractile activity in the tubular esophagus and incomplete relaxations of the lower esophageal sphincter
diagnosis • the diagnosis of achalasia.
In view of her comorbidity, she initially underwent local therapy with botulinum toxin, which did not lead to symptomatic improvement. • Therefore, a balloon dilation was performed, alleviating her pulmonary and esophageal symptoms.
Discussion • More recently, extraintestinal manifestations of esophageal diseases have attracted significant attention. • Due to its high prevalence reflux disease is probably the most common esophageal cause for laryngeal or tracheo-bronchial problems. • However, patients with achalasia are at much higher risk for passive regurgitation with aspiration.
Camara et al. found evidence for pneumonia at the time of autopsy in about one third of patients with megaesophagus. • Dysphagia or other esophageal symptoms may be overlooked as patients adjust to the chronically impaired swallowing function and focus on the more acute symptoms related to pulmonary complications.