Download
1 / 16
410 likes | 1.22k Views
T Cell Receptor Excision Circle (TREC) Assay for Newborn Screening of SCID. Francis K. Lee, M.Sc , Ph.D. Senior Service Fellow (Research Microbiologist) Newborn Screening Translation Research Initiative, CDC Emeritus Professor of Pediatrics, Emory University School of Medicine .

E N D
T Cell Receptor Excision Circle (TREC) Assay for Newborn Screening of SCID Francis K. Lee, M.Sc, Ph.D. Senior Service Fellow (Research Microbiologist) Newborn Screening Translation Research Initiative, CDC Emeritus Professor of Pediatrics, Emory University School of Medicine Newborn Screening Molecular Workshop June 28-30, 2011 National Center for Environmental Health · Division of Laboratory Sciences Newborn Screening and Molecular Biology Branch
Overview of SCID – the Condition • Severe Combined Immunodeficiency (SCID) is characterized by the absence of both humoral and cellular immunity • At least 15 different genes known to cause SCID when mutated • All have profound defects in T lymphocyte differentiation and function • Maternal antibodies wane during first months of life - affected infants develop infections (common / opportunistic pathogens) • Recurrent infections, chronic diarrhea, sepsis, FTT • Death usually before 1 year of age • Treatment and prevention of infections can prolong life but are not curative • Best hope for SCID patients is Hematopoietic Stem Cell Transplant before the onset of infections SCID has been called “Bubble Boy Disease”
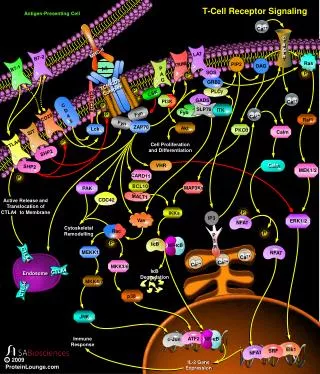
X-linked SCID: Mutation in the γ chain common to IL-2, IL-4, IL-7, IL-9, IL-17 & IL-21 receptors Autosomal Recessive SCID: Adenosine Deaminase deficiency (20q13.11) Jak3 tyrosine kinase deficiency (19p13.1) RAG 1 or 2 defect (11p13) IL-7R deficiency ( chain) (5p13) SCID classification • Purine Nucleoside Phosphorylase deficiency (14q13) • MHC II deficiency (16p13, 1q21, 13q) • CD3 and CD3 mutations (11q23) • CD45 deficiency • ZAP-70 deficiency- (2q12) • Artemis (10p)
Mutations in IL2R gamma chain NHIGRI, NIH: Genbank accession number L19546
TRECs: Reduced in All Forms of SCID Common Feature: ABSENT/NON-FUNCTIONAL T CELLS IL2R T- B+ NK- JAK3 T- B+ NK- IL7R T- B+ NK+ CD45 T- B+ NK+ RAG1 T- B- NK+ RAG2 T- B- NK+ ARTEMIS T- B- NK+ ADA T- B- NK- Reticular Dysgenesis T- B+ NK+ SCID, multiple bowel atresiasT- B+/- NK+ SCID, congenital abnormalities T- B+/- NK+ Severe DiGeorge Syndrome T- B+/- NK+ CD3 Deficiency T+/- B+ NK+ CD8 Deficiency T+ B+ NK+ Severe Ataxia TelangiectasiaT+/- B+/- NK+ Unknown genetic Defect ~5-25%
SCID Meets NBS Criteria • Prevalence of the disease 1:100,000 or greater • SCID: 1:50,000-1:100,000 • Can the disorder be detected by routine physical exam? • SCID: Baby appears normal at birth. • Does the disease cause serious medical complications? • SCID: 100% fatal within the first year of life • Is there a cheap, sensitive and specific screening test? • SCID: Real time PCR to enumerate T cell receptor excision circles • Is there a confirmatory test? • SCID: Lymphocyte subpopulation analysis • Does early detection improve outcome? • SCID: Early HSCT decreases mortality from SCID
Optimal Test to Screen for severe T cell lymphopenia (SCID) • Must detect low/absent T cells • Use existing NBS screening cards • Inexpensive, sensitive and specific • Low rate of false positive tests • Little need for retesting • Real Time PCR (RT-PCR): enumeration of T cell receptor excision circles (TREC - surrogate marker for recently produced T cells) using DNA extracted from newborn blood spots collected routinely on all newborns
Overview of TREC Assay for SCID • The T cell Receptor Excision Circle (TREC) assay differs from other molecular assays used in NBS: • Phenotype assay: TREC is a molecular marker for T cell production in thymus • Quantitative assay: require higher level of precision • results influence d by • DNA extraction efficiency • PCR efficiency
Overview of TREC Assay for SCID (cont.) • T cell receptor excision circles (TREC) are by-products of the rearrangement of T cell receptor (TCR) genes during thymocyte maturation in the thymus • TRECs are episomalDNA and do not replicate during mitosis • Peripheral blood TREC levels reflect T lymphocyte production in the thymus • TREC Assay: Real Time PCR • Variations in TREC Assay procedures can be based on: • Primers and Probes • DNA extraction procedures
TCR–Delta deletion in rearrangement of T cell receptor gene Vδ/Dδ/ Jδ Vαn Jαn Cδ Cα Vδ1 ψЈα Jα1 Jα3 Vα1 Vα2 δRec Jα2 ≈ ≈ Chromosomal 14 TCR α/δchain loci ≈ ≈ Alpha chain V segments Delta chain V/D/J segments Alpha chain J segments Alpha chain constant region ↓ ≈ Chromosomal 14 TCR α/δchain loci ≈ ≈ ≈ ↓ Signal joint ≈ δRec-ΨJα TREC Episomal DNA (δRec-ΨJα TREC) Chromosomal 14 TCR αchain locus ≈ ≈ ≈ δRec-ΨJα Coding joint ↓ Vα–Јα–Cα rearrangement ↓ TCR alpha chain transcription, translation , expression
Orientation of δRec and ΨЈα sequences in genomic DNA δRec ΨЈα ≈ GTGTCCTCACCCGTGAAA 5’ 3’ GTCCACGGATACGTAGTGGCAC Orientation of δRec and ΨЈα sequences in TREC DNA ≈ Signal Joint 5’ -------AAAGGTGCCCACTCCTGTGCACGGTGATGCATAGGCACCTG-------3’ Forward Primer Direction → ← Reverse Primer Direction
Technical Approaches to TREC Assays Classical Conventional CDC PE DBS DNA Extraction DBS DNA Extraction DBS In Situ Real time PCR DBS In Situ PCR TREC sequence Amplification Real time PCR Amplicons Quantification Amplicons Quantification
Dried blood spots (DBS) Enumerate TRECs by real-time qPCR Extract DNA* 96 well plate 3 mm punch NBS Card TREC Measurement: qPCR
In Situ Real Time PCR Assay for TREC Punch one 2.0 mm discs from DBS specimen into PCR tubes Wash with 125 µl of DNA purification solution S1 (shake for 15 minutes at room temp) Wash with 125 µl of DNA elution solution S2 (shake for 5 minutes at room temp)
In Situ Real Time PCR Assay for TREC (cont.) Discard S2 wash buffer Add 15 μl of qPCRmastermix (contains complete mix of primers & probe) Run qPCR in StratageneMX3000p: 45 deg for 5 min, 95 deg for 20 min 45 cycles of [ 95 deg x 15 sec + 60 deg x 1 min ]
Quality AssuranceUse of TREC Reference Materials National Center for Environmental Health Newborn Screenand Molecular Biology Branch