Download
1 / 1
10 likes | 133 Views
This study utilizes the extensive ACCENT database to develop new prognostic nomograms that predict overall survival (OS) and time to recurrence (TTR) for patients with Stage III colon cancer. By analyzing 15,995 patients, the nomograms incorporate a wide array of patient characteristics, improving risk stratification compared to traditional AJCC v7 staging. The final models demonstrated robust internal validation, suggesting their potential utility in clinical decision-making and patient communication, optimizing treatment strategies and prognostic understanding.

E N D
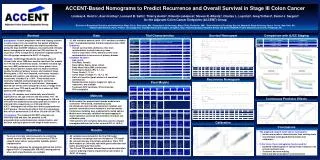
ACCENT-Based Nomograms to Predict Recurrence and Overall Survival in Stage III Colon Cancer Lindsay A. Renfro1, Axel Grothey2, Leonard B. Saltz3, Thierry André4, Roberto Labianca5, Steven R. Alberts2, Charles L. Loprinzi2, Greg Yothers6, Daniel J. Sargent1 for the Adjuvant Colon Cancer Endpoints (ACCENT) Group 1Division of Biomedical Statistics and Informatics, Mayo Clinic, Rochester, MN; 2Department of Oncology, Mayo Clinic, Rochester, MN; 3Gastrointestinal Oncology Service, Memorial Sloan-Kettering Cancer Center, New York, NY; 4Hôpital Saint Antoine, Paris, France; 5Oncology Unit, Ospedali Riuniti di Bergamo, Bergamo, Italy; 6National Surgical Adjuvant Breast and Bowel (NSABP) Project Biostatistical Center, Pittsburgh, PA Abstract Data Trial Characteristics Survival Nomogram Comparison with AJCC Staging Background:Current prognostic tools and staging systems in colon cancer (CC) use relatively few patient attributes; including additional covariates may improve prediction. Using the large ACCENT database, we constructed clinically based nomograms for overall survival (OS) and time to recurrence (TTR) in stage III CC that better separate patients into risk groups compared to AJCC v7 staging. Methods:15,995 stage III patients accrued to phase III clinical trials since 1989 were used to construct Cox models for TTR and OS, stratified by study. Variables included age, sex, race, BMI, performance status, tumor grade, tumor stage, ratio of positive lymph nodes to nodes examined, number/location of primary tumors, and treatment class. Missing data (<18%) were imputed, continuous variables modeled with splines, and clinically relevant pairwise interactions included if p < 0.001. Final models were internally validated via bootstrapping for corrected calibration and C-indices for survival data. Nomogram-defined risk tertiles were compared to AJCC v7 stage III for observed 3-year TTR and 5-year OS for a subset of 7400 patients with complete data. Results:All variables were statistically and clinically significant for OS; age and race did not predict TTR. No meaningful interactions existed. Nomograms for OS and TTR were well calibrated and associated with C-indices of 0.66 and 0.65, respectively, vs. 0.58 and 0.59 for AJCC. Nomogram risk tertiles were better separated than AJCC groups. Removing treatment from the nomograms did not hurt performance (C=0.66 for OS and 0.65 for TTR). Conclusions:The proposed ACCENT nomgrams are internally valid and have the potential to aid prognostication, patient/physician communication, and decision making in patients with stage III colon cancer. • 15, 936 individual patients (with > 50% variables available) from 12 randomized phase III trials conducted since 1989 • Endpoints: • Overall survival (OS), defined as time from randomization to death from any cause • Time to recurrence (TTR), defined as time from randomization to recurrence of primary disease • Candidate Variables: • Age (years) • Sex (Male, Female) • Race (White, Black, Asian, Other) • Body Mass Index (BMI; continuous) • Performance Status (PS; 0, 1, 2+) • Tumor Grade (1, 2, 3+) • Tumor Stage (T-stage; T1, T2, T3, T4) • Ratio of # positive lymph nodes to # examined (continuous) • Number/location tumors: single left, right, or transverse; any multiple • Treatment (5FU Variations, 5FU+irinotecan, 5FU+oxaliplatin) Recurrence Nomogram Final Models Methods Continuous Predictor Effects • Multivariable Cox proportional hazards models were created for TTR and OS, stratified by study • All statistically and clinically significant variables and pairwise interactions were included in the final models • Continuous variables were modeled with nested splines • Models were internally validated via bootstrapping to obtain optimism-corrected discrimination (C-index) and calibration plots • 7,400 patients with complete data were used to compare nomogram-defined risk tertiles versus AJCC v7 (A,B,C) Calibration Conclusions Objectives Results • The proposed stage III colon cancer nomograms: • Involve more patient characteristics than existing tools • Are internally valid (good discrimination and calibration) • In the future, these nomograms may be used for: • Stratified randomization in clinical trials to balance risk across treatment arms • Treatment decision-making • Enhanced physician/patient communication • To create internally valid nomograms for predicting overall survival (OS) and time to recurrence (TTR) in stage III colon cancer using widely available patient characteristics • To compare outcomes by nomogram-defined risk tertiles against AJCC v7 staging (IIIA, IIIB, IIIIC) among patients where both classifications are available • All variables were included in the final OS model • All variables except age and race included in TTR model • No relevant two-way interactions existed for OS or TTR • Both models are internally valid with good calibration and better discrimination than AJCC • The OS and TTR models showed improved discrimination (correct ordering of pairs of patients by risk) relative to AJCC v7 staging


















