Download
1 / 41
770 likes | 2.13k Views
Foot and Ankle Pain. Prof. Dr. Ece AYDOĞ Physical Medicine and Rehabilitation. The ankle , or tibiotalar , joint comprises the articulation between the foot ( talus ) and the lower leg ( distal tibia and fibula ). FUNCTIONAL ANATOMY AND BIOMECHANICS.

E N D
Foot and Ankle Pain Prof. Dr. Ece AYDOĞ Physical Medicine and Rehabilitation
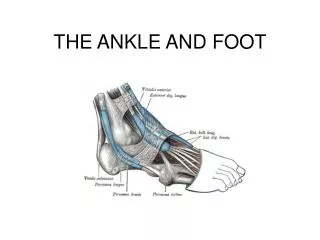
The ankle, or tibiotalar, joint comprises the articulation between the foot (talus) and the lower leg (distal tibia and fibula). FUNCTIONAL ANATOMY AND BIOMECHANICS
Forefoot; toes and metatarsal bones; metatarsophalangeal (MTP) and interphalangeal joints Midfoot; tarsometatarsal (TMT) joints connect the forefoot to the midfoot, which comprises the three cuneiform bones, the navicular, and the cuboid Hindfoot;talus and calcaneus, talocalcaneal (subtalar), talonavicular, and calcaneocuboid articulations. Anatomic regions
PHYSICAL EXAMINATION • Location of swelling • Deformity; • Hallux valgus or bunion • Hammer toes, • Flatfoot deformity (characterized by hindfoot valgus/forefoot abduction). • Callosities • Rheumatoid nodules • Ulcerations • Wear patterns: “A deformed foot can deform any good shoe; in fact, in many cases the shoe is a literal showcase for certain disorders.”
Gece Ateli Hallux Valgus
Rheumatoid nodules Diabetic ulcer
PHYSICAL EXAMINATION • Metatarsal heads and MTP joints palpation in patients with RA or nonarthritic metatarsalgia; tenderness, synovitis, and swelling. • Tenderness over the posterior aspect of calcaneus; Achilles tendinitis • Pain over the medial tubercle (palpable on the medial plantar surface); plantar fasciitis. • Tenderness over sinus tarsi of the hindfoot (located laterally, just anterior and distal to the tip of the fibula); talocalcaneal joint pathology • Tenderness over the anterior joint line usually correlates with ankle joint pathology.
Calcaneal medial tubercule (Plantar fasciitis) Talocalcaneal yoint pathology
Range of motion analysis: 10 to 20 degrees of dorsiflexion 40 to 50 degrees of plantar flexion. PHYSICAL EXAMINATION
Normal hindfoot inversion and eversion are each approximately 5 degrees.
COMMON CAUSES OF ANKLE PAIN ANTERIOR AND CENTRAL ANKLE PAIN • Spur and osteophyte formation • Arthritis (degenerative or inflammatory) • Anterior tibial tendon tendinitis or tendinosis • Stress fractures • Osteochondral defect
in most instances, Achilles pain results from degenerative tendinosis, with or without an overlying tendinitis. associated intratendinous spur formation is common spur excision also frequently entails tendon débridement, reconstruction, and transfer. POSTERIOR JOINT PAINAchilles tendon
protected by two distinct bursae. more superficial bursa is immediately subcutaneous and becomes inflamed primarily with irritation from ill-fitting shoes with a tight counter (“pump bump”). Achilles tendon
“retrocalcaneal” bursa is a larger structure that lies deep to the Achilles tendon. Inflammation of this structure often accompanies Achilles tendinitis/tendinosis. It also may be irritated by an enlarged posterior superior calcaneal tuberosity, sometimes referred to as a Haglund's deformity. Achilles tendon
MEDIAL ANKLE PAIN • Stress fracture • Arthritis • Inflammation or degeneration (or both) of the posteromedial flexor tendons, including the posterior tibial tendon and the flexor hallucis longus and flexor digitorum longus tendons • long-standing synovitis and dysfunction of posterior tibial tendon ultimately may lead to collapse of the arch and the development of an acquired flatfoot deformity.
Tarsal tunnel syndrome is another cause of posteromedial ankle pain. pain that radiates into the plantar foot percussion of the tarsal tunnel reproduces these symptoms (Tinel's sign). MEDIAL ANKLE PAIN
LATERAL ANKLE PAIN • Stress fracture • Arthritis • Peroneal tendon pathology; • tenosynovitis • longitudinal “split” tears • chronic tendon instability • the tendons sublux over the posterolateral edge of the fibula, causing pain and attritional tearing
COMMON CAUSES OF FOOT PAIN FOREFOOT PAIN • The forefoot region is a common location of foot pain.
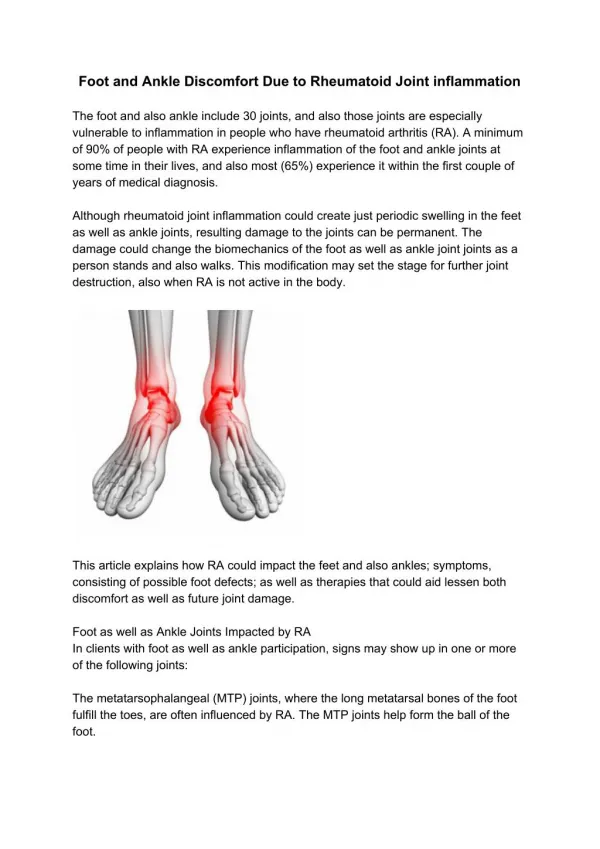
inflammation and progressive MTP synovitis eventually lead to capsular distention and destruction. loss of collateral ligament stability and, finally, destruction of the articular cartilage and bone Rheumatoid Arthritis
FOREFOOT PAIN • Hallux valgus deformity or bunion; • commonly encountered in patients with and without inflammatory arthritis • RA; 70% • progression of this deformity may be accelerated further by loss of support from the adjacent lesser MTP joints. • Hallux rigidus • Degenerative arthritis • Sesamoiditis • Osteonecrosis • Fracture
FOREFOOT PAIN • Claw toes • Hammer toes • Mallet toes • Etiologies; • arthritis, • trauma, • nerve/muscle imbalance, • and chronic use of shoes with inadequate toe boxes. • Instability; • mechanical causes (long second metatarsal) • inflammatory disease • MTP joint subluxation
Claw toe • Mallet finger
FOREFOOT PAIN Metatarsalgia • Gastrocnemius contracture or tight Achilles tendon; the forefoot is prematurely loaded during the stance phase of gait. • Hammer toes and mallet toes can result in downward pressure on the metatarsal heads, leading to metatarsalgia. • In elderly patients and patients with inflammatory arthritis, atrophy of the plantar fat pad of the forefoot also can result in metatarsalgia.
Morton's neuroma: between the third and fourth metatarsal heads burning, aching, or shooting pain symptoms are especially exacerbated with tight shoes . LATERAL FOREFOOT
Bunionette: angular deformity of the fifth toe pain over the lateral aspect of the fifth metatarsal head LATERAL FOREFOOT
MIDFOOT PAIN • Arthritis at the TMT joints • most frequently the first TMT joint on the medial side of the foot • instability of the first TMT joint, repetitive stress can lead to dorsiflexion of the first metatarsal • midfoot arthritis can lead to an abduction deformity of the foot, where the forefoot and metatarsals deviate outward.
MIDFOOT PAIN • lateral midfoot pain: • peroneal tendinitis • stress fracture of the fifth metatarsal • medial midfoot pain: • accessory navicular bone • osteonecrosis of the native navicular bone • insertional posterior tibial tendinitis
HINDFOOT PAIN • joints of the hindfoot • talonavicular • talocalcaneal • calcaneocuboid • degenerative and inflammatory arthritis • RA; 21% to 29% • posterior tibial tendinitis and dysfunction • Inflammation • Degeneration • Dysfunction
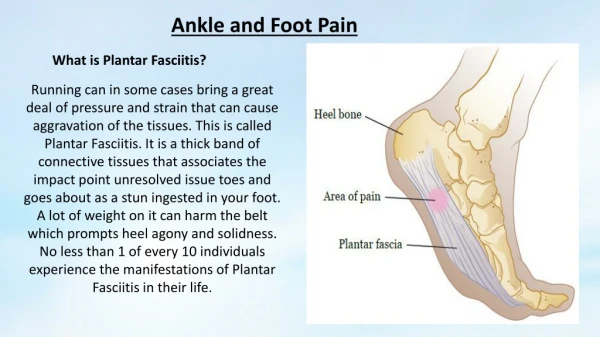
HEEL PAIN • Plantar fasciitis; • inferior heel pain • worse when first getting up in the morning or getting up after sitting for a long time • Achilles tendinosis; • posterior heel pain • worse during or after exercise • Nerve entrapment; • first branch of the lateral plantar nerve (Baxter's nerve) • medial heel pain • Calcaneal stress fracture; • medial and lateral pain • Calcaneal stress fracture usually can be distinguished by a positive “squeeze test,” with compression of both sides of the heel.
NONOPERATIVE TREATMENT • Medicalmanagement • Nonsteroidal anti-inflammatorydrugs • Steroids • Disease-modifyingantirheumaticdrugs
NONOPERATIVE TREATMENT • Shoewear modification • deep, wide toe box • firm heel counter • soft heel • Well-constructed walking or jogging shoes usually provide sufficient room for mild-to-moderate deformities
NONOPERATIVE TREATMENT • Often it is necessarytoprescribe a customorthotic insertforpatientswithmoremoderatedeformities • It is typicallynecessarytoremovetheinsole of theshoetomakeroomfortheorthotic insert • Customorthoses; • rigid, • semirigid, • softeraccommodativedevices • Rigidandsemirigidorthosesusuallyareusedtocorrectsuppledeformitiesandshould be usedwithcaution in patientswitharthritis • Mostwalkingor jogging shoessuffice.
NONOPERATIVE TREATMENT • More commonly, these patients, especially if they have RA, benefit from accommodative orthoses (i.e., orthoses made of softer material that can be molded to “accommodate” a deformity) • Accommodative orthoses can be modified further by incorporating a “relief” under a deformity, further unloading it • When sending patients for orthoses, it is best to provide the orthotist with a prescription that includes the patient's precise diagnosis (e.g., metatarsalgia) and the type of orthosis and any modifications desired (e.g., a “custom accommodative orthosis with a relief under the lesser metatarsal heads”).
Injections • Mixture of anestheticandcorticosteroid • Injection of a corticosteroidnearordirectlyinto a tendon can adverselyaffectthebiomechanicalproperties of thetendon, ultimatelyleadingtorupture • AvoidcorticosteroidinjectionsintothelesserMTPswhenthere is evidence of jointinstability. • Suchinjections can leadtofurtherattenuation of thejointcapsuleandresult in frank jointdislocation.
OPERATIVE TREATMENT • If symptoms persist despite nonoperative management, surgical intervention should be considered • Arthrodesis (joint fusion), • Arthroplasty (joint replacement), • Corrective osteotomy, • Tendon débridement and transfer, • Synovectomy (joint or tendon).