Download
1 / 65
800 likes | 1.78k Views
Diabetic foot and ankle. Marie-france rancourt november 2012. outline. Diabetes Evaluation and Work Up Charcot Diabetic Ulcers Case OITE Questions. diabetes in canada. 2 359 252 people with diagnosed diabetes 6.4% of the population 3rd highest prevalence in the World (USA, Portugal)

E N D
Diabetic foot and ankle • Marie-france rancourt • november 2012
outline • Diabetes • Evaluation and Work Up • Charcot • Diabetic Ulcers • Case • OITE Questions
diabetes in canada • 2 359 252 people with diagnosed diabetes • 6.4% of the population • 3rd highest prevalence in the World (USA, Portugal) • 9.6% Overweight (BMI average = 29) Source: Public Health Agency of Canada (July 2011)
presentation • Incidental finding • Bloodwork • Xrays • Foot monitoring in diabetics • Swelling • Ulcers • Pain
diabetic neuropathy • The gold standard : Nerve conduction studies • Semmes-Weinstein monofilament test • 10g of pressure with 5.07 nylon • Most commonly used • Sensitivity of 91% • Specificity of 86% • 128-Hz tuning fork • Vibration testing • More sensitive predictor of early neuropathy
diabetic vasculopahty • Palpation of pulses • If pulses absent, further tests... • Ankle-Brachial Index • < 0.4-0.5: poor wound healing • Transcutaneous oxygen pressure measurements (TcpO2) • Measures partial pressure of O2 diffusing through the skin • > 40mmHg: good wound healing potential • < 30mmHg: poor wound healing potential • CT angio
work up • CBC, lytes, BUN, Cr • Infection work up • ESR, CRP • Bone Scan • Technetium: may be misleading • Indium: cold for neuropathy and hot for osteomyelitis (sensitivity 93%, specificity 80%) • MRI: osteomyelitis • RBS, HBA1C • HBA1C more than 0.08 = poor wound healing • Albumin (malnourishment<3.5 g/dL))
jean-marie charcot • 1825-1893 • French neurologist • 1868 - Tertiary Syphilis • Charcot-Marie-Tooth, Multiple Sclerosis, Parkinson’s, Hysteria • Pupils • Sigmund Freud • George de la Tourette • Joseph Babinski
Une leçon clinique à la Salpêtrière - André Brouillet - 1887
definition • Chronic progressive destruction of joint following loss of protective sensation • Neuropathic arthropathy • Diabetes and Charcot • 0.4% of patients with diabetses • 7.5% of patients with diabetes + neuropathy • Monitor other foot (involved in 9-35%)
pathomechanism • Neurotrauma: • Loss of peripheral sensation and proprioception • Repetitive microtrauma • Inflammatory resorption of traumatized bone • Neurovascular: • Dysregulated autonomic system • De-sensitized joints receive significantly greater blood flow • Hyperemia leads to increased blood flow and metabolism • Osteoclastic resorption of bone • Osteopenia
presentation • Type 1 Diabetes: in fifth decade (20-24 yrs post onset) • Type 2 Diabetes: in sixth decade (5-9 yrs post onset) • Swollen • Warm (may be up to 3 degrees warmer than contralateral side) • Pain (50%) • Erythematous • Unstable • Mimics infection • Elevate the affected limb
Brodsky’s anatomicclassification • Type 1 • Most common (60%) • Rocker bottom foot • Valgus • At risk for ulcers • Type 2 • 10% • Unstable, long immobilization • Type 3 A • 20% • Ulcerations/Osteomyelitis over malleoli • Type 3 B • Post calcaneal fractures
treatment van der Ven et al. (JAAOS, 2009)
non surgical treatment • Total Contact Casting • 75% success • Q2wks • 4 months (forefoot-midfoot) to 1 yr (hindfoot-ankle) • Non weight bearing vs protected weight bearing • Appropriate footwear and insole • CROW • Bisphosphonates
surgery • Eichenholtz Stage 3 • Arthrodesis • High complication rate • Up to 69% • Infection, hardware failure, ulcerations, fractures • Long time to fusion (11-22 wks) • NWB x 3 months • External fixation • Dynamic ring • Total ankle arthroplasty contraindicated • Amputation (2.7% annual rate)
Long-term follow-up of tibiocalcaneal arthrodesis in diabetic patients with early chronic Charcot osteoarthropathy.Caravaggi CM et al.J Foot Ankle Surg. 2012 Jul-Aug;51(4):408-11. doi: 10.1053/j.jfas.2012.04.007. Epub 2012 May 26. • Arthrodesis in the coalescence or remodeling (subacute and chronic) stages of the disease before the onset of joint instability, severe deformity, and ulcer formation. • Observational study • 45 diabetic patients • Mean follow-up duration of 5 ± 2.85 years • 39 (86.67%) patients returned to independent ambulation wearing custom-made shoes with molded insoles • 2 (4.44%) others required pneumatic casts for ambulation. • 2 (4.44%) others underwent below-the-knee amputation shortly after the ankle arthrodesis because of postoperative infection
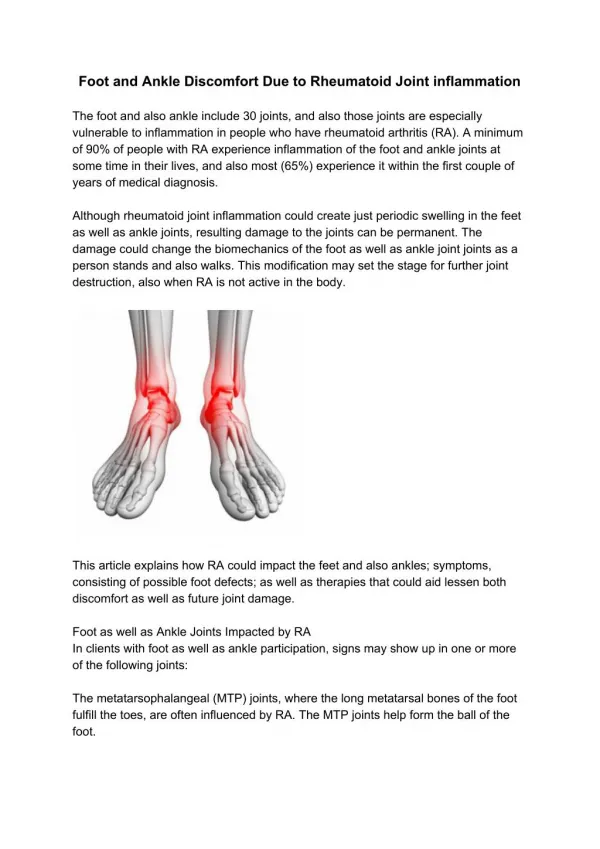
presentation • Seen in 10-15% of diabetic patients • 10-20% of ulcers develop into osteomyelitis
pathophysiology • Autonomic dysfunction • Lack of glandular function • Dry Skin • Skin more prone to stress • Lack of sensory protective mechanism • Decrease of healing blood supply
mechanics • Tight Achilles tendon • Plantarflexion deformity • FOREFOOT Pressure Malalignment Bone Loss HINDFOOT Pressure Vascular Insufficiency Architectural collapse (cuneifrom, cuboid) MIDFOOT Pressure Skin breakdown
treatment Anakwenze et al. (JAAOS, 2012)
non-operative treatment • Antibiotics • Started post cultures • Custom made Orthotics • Rocker soles to relieve forefoot pressure • Total Contact Casting • Wagner grade 1 & 2 (in absence of osteomyelitis) • 4 - 6 weeks of treatment
surgical treatment • Correction of deformity or pressure point • Forefoot: • I & D • Achilles tendon lenghtening • Syme amputation • Midfoot: • resection of offending bone (Brodsky 1) • Realignement fusion if recurring ulceration and unbracable deformity • Hindfoot: • Partial calcanectomy • Sural fasciomusculocutaneous free flap • BKA
syme amputation • patent tibialis posterior artery • more energy efficient than midfoot even though it is more proximal • stable heel pad is most important factor
Syme Ankle Disarticulation in Patients with DiabetesBY MICHAEL S. PINZUR (JBJS 2003) • 97 adult patients with diabetes mellitus • Retrospective • 84.5% ultimately achieved wound-healing • vascular inflow (ultrasound Doppler ischemic index of 0.5 or transcutaneous partial pressure of oxygen between 20 and 30 mm Hg) and tissue nutrition (serum albumin of 2.5 g/dL) were met • The overall infection rate was 23%, and it was three times greater in smokers. • Minimum 2years follow up all but 2 patient walked with a prosthesis • 31 patients died at an average of 57.1
Below knee amputation • Pre operative physiatry consult • Walking energy expenditure increases by 25-40% • Surgery • Incision: post flap longer than ant flap • Level: junction of proximal and middle third of tibia, below tibial tubercle, 15cm below medial joint line, fibula 2cm shorter than tibia • Bone cuts: transverse and beveled • Avoid periosteal stripping (avoid HO, synostosis) • Nerves: identify, gentle traction, injection of local, sharply transected • Vessels: tie on both sides (2 prox and 1 distal) • Larger posterior flap to bring over • Incision closure: more anterior than distal, no tension
Below knee amputation • Post op • Cast vs Dressing • Keep dressing on for around 5 days • Suture removal • Medical comorbidity management, good diet
A Comparison of Rigid vs Soft Dressings in the Healing of Below Knee Amputations (BKA)Journal of Vascular Surgery (November 2012), 56 (5), pg. 1479-1479Shine et al. • We hypothesized that rigid dressings would facilitate faster wound healing and residual limb maturation by minimizing postsurgical edema and pain, preventing knee flexion contracture, and protecting the residual limb from trauma. • Methods: Our retrospective analysis compared 151 patients (2000 to 2012) at Yale New Haven Hospital, after which • 60 patients received soft dressings and knee immobilizers (soft) • 92 were placed in a rigid plastic or plaster prosthesis (rigid). • Results: Age and diabetic status was not statistically different between the soft (61.0 years, 82.8% with diabetes) and rigid groups (58.6 years, 78.0% with diabetes). • After 60 days, 58.24% of the rigid group was cast vs 38.33% of soft group
cases • Pace, Trina 35995299 • Venables, Laura 10097442 • Lajeunesse, Michelle 09442948
L.V. 10097442 • 81 yo lady • Past medical history: Diabetes mellitus with neuropathy, right total knee arthroplasty, hypertension • Allergies: Penicillin with rash • Social history: Nonsmoker, no EtOH • Medications: Lasix, metformin, insulin, amlodipine, pantoprazole, Lipitor, Celebrex
surgeries • 2003: necrotic 3rd toe dislocation • right 3rd toe amputation • 2009: Rocker bottom neuropathic foot, plantar ulcer, Achilles tendon contracture • Midfoot medial closing wedge osteotomy • Mid tarsal fusion • Achille tendon lenghtening: percutaneous triple hemisection
Progression - 2012 • Valgus deformity of the ankle • Lateral tilt of tibial plafond • Swelling • Minimal pain • No ulcers • Neuropathy, good pulses
surgeries • 2012: Right ankle Charcot • Right ankle arthrodesis • Right subtalar arthrodesis • Procedure • Direct lateral and posteromedial approach • Remove distal 8 cm of fibula • Medial malleolus osteotomy • Distal tibia and talar dome osteotomy • Slight ER, Valgus • Wright Medical Valor Nail + 7.3mm screw
Post arthrodesis • 2 ulcers with purulent discharge: ankle + plantar surface • No cultures • Ciprofloxacin x 2 weeks then Keflex x 3 months • No systemic symptoms. • Diabetes is well controlled • Followed by ID, Wound Care • Hardware removal at around 6 months