Download
1 / 28
280 likes | 461 Views
CONGENITAL SYPHILIS. SINDHU E. PHILIP, MD. DEPARTMENT OF PEDIATRICS 09/20/02. Introduction. Infant usually infected in utero by transplacental passage of Treponema pallidum from infected mother at any time. Infection may also occur from contact with an infectious

E N D
CONGENITAL SYPHILIS SINDHU E. PHILIP, MD. DEPARTMENT OF PEDIATRICS 09/20/02
Introduction Infant usually infected in utero by transplacental passage of Treponema pallidum from infected mother at any time. Infection may also occur from contact with an infectious lesion during passage through the birth canal It remains unclear what factors determine which mothers, particularly those in the latent stage, will pass the disease to the fetuses. Also unclear why some infants, infected in utero, are born asymptomatic, but develop overt dz. In first few wks./mo.
Epidemiology • Worldwide, but more frequent in urban areas. • Incidence of congenital syphilis has dramatically decreased • in the U.S. since 1991.
Infection can be transmitted to fetus at any stage of disease. • Rate of infection 60% - 100% during second stage. • Transmission rates slowly decreases with increasing duration of the disease. • Women, untreated early syphilis: 40% • of pregnancies result in spontaneous abortion, stillbirth, or perinatal death.
Pathogenesis Infection before 4th month of pregnancy? Possible that treponemes do in fact pass from mother to fetus before 5th month of gestation, but classic pathologic changes do not occur until after 5th month. Infection involves the placenta, and spreads hematogenously to the fetus, widespread involvement is characteristic. Infected placenta is paler, thicker, and larger than normal.
Clinical Manifestations • Damage to fetus depends on the stage of development • at which infection has taken place and time elapsed • before treatment. • Early infection, untreated: miscarriage, stillbirth, neonatal • death, IUGR, premature delivery. • Survivors: • Early congenital syphilis: clinical manifestations within first • 2 years of life • Late congenital syphilis: clinical manifestations after 2yo.
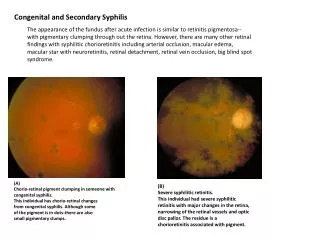
Hepatosplenomegaly- diffuse inflammation, scarring Jaundice – due to hepatitis Generalized lymphadenopathy –epitrochclear nodes Coombs – hemolytic anemia, thromobocytopenia, leukopenia, leukocytosis Hydrops fetalis Mucocutaneous:rhinitis (highly infectious), “snuffles”, mucous patches Macuolpapular rash Desquamation Pemphigus syphiliticus (vesicular bullous eruptions of palms and soles) Petechial lesions Bony lesions, osteochondritis, periostitis, pseudoparalysis Syphilitc leptomeningitis Chorioretinitis,salt and pepper fundus, glaucoma Pancreatitis Early Congenital Syphilis Early manifestations are varied, with multi-system Involvement
Broken vesicles, desquamation Condylomata around anus Infiltration, desquamation and rhinitis
Rhinitis (snuffles), mucous patches, damage to palate(late) Bullae and vesicular rash on soles Eroded papular lesions
Lone Bone Radiographs Osteochondritis of distal radius and ulna Osteochondritis of femur and tibia metaphysis
Interstitial keratitis (inflammatory) Nerve deafness Clutton’s Joints (synositis, restricted movement) Hutchinson’s triad (teeth, intersitial keratitis, 8th nerve deafness) Mulberry molars Flaring scapulas Hydrocephalus Mental retardation Frontal bossing Saddle nose Protruding mandible High arched palate Perioral fissures Higouemenaki’s sign(periosteal rxn of clavicle, sternocleidomastoid) Saber shins Rhagades (linear scars that become fissured or ulcerated) Late Congenital Syphilis Results primarily from chronic inflammation of bone, teeth, and CNS.
Hutchinson’s teeth – peg shaped upper incisors Frontal Bossing
Saber shins: Anterior bowing of tibias Gumma: Thin atrophic scar
Diagnosis Definitive diagnosis can be made by dark-field microscopy on specimen from skin lesions, placenta, umbilicus. • Serologic tests are the principal means for diagnosis: • Nontreponemal test: VDRL, RPR • Treponemal tests: TPI, FTA-ABS, MHA-TP
Diagnosis • Nontreponemal: VDRL, RPR • Quantitative results correlate with disease activity, • therefore helpful in screening. • Titers rise when disease is active, fall when treatment is adequate • In congenital infxn. These tests become non- reactive • within a few months of adequate treatment.
Non-treponemal testing • Detects antibodies against a cardiolipin- cholestrol- lecithin complex, not specific for syphilis. False Positives: Only in serum, not in CSF testing • certain viral infxns: infectious mononucleosis, hepatitis, varicella, measles • lymphoma, TB, malaria, endocarditis, • connective tissue disease • pregnancy (?) • abuse of injection drugs
Diagnosis • A sustained 4 fold decrease in titer of nontreponemal • test after treatment demonstrates adequate therapy. • A 4 fold increase titer increase after treatment suggests • reinfection or relapse.
Confirmatory Testing Treponemal Tests: TPI, FTA-Abs, MHA-TP Treponemal antibody titers become positive soon After initial infection and usually remain positive For life, even with adequate therapy. Antibody titers do not correlate with disease activity, and are not quantified. Not 100% specific for syphilis: other spirochetal dz,
Infant Testing Reactive serology in neonate could be due to IgG passively transferred to newborn through placenta, and does not indicate active infection. If infant’s titer higher than mother’s congenital infection If decreasing titer in infant passive transfer of antibodies, should disappear by 3-4 months of age. Persistently reactive VDRL, with rising titer Active Infection
Non-treponemal Test(VDRL, RPR, EIA, ART) Treponemal Test(MHA-TP, FTA-ABS) Mother Infant Mother Infant Interpretation - - - - No syphilis or incubating syphilis in the mother and infant. + + - - No syphilis in mother (false-positive non-treponemal test with passive transfer to infant). + +/- + + Maternal syphilis with possible infant infection; or mother treated for syphilis during pregnancy; or mother with latent syphilis and possible infection of infant. + + + + Recent or previous syphilis in the mother; possible infection in the infant. - - + + Mother successfully treated for syphilis before or early in pregnancy; or mother with Lyme disease, yaws, or pinta (ie, false-positive serology). Recommended Interpretation
CSF Examination CSF abnormalities may occur in congenital syphilis Even in absence of neurologic involvement. * Leukocytosis * Elevated protein in CSF * positive VDRL (no false positives)
Maternal hx, results of serologic testing Thorough P.E. Long bone xrays Non-treponemal AB titer Treponemal AB titer Head US Csf Analysis for VDRL, cell count & protein CBC with platlets LFT’s UA Chest xray HIV antibody test Opthalmologic exam Evaluation
Treatment Proven or highly probable: Aqueous crystalline Penicillin G 100,000-150,000U/kg/day (given q8-q12hrs) IV for 10 days OR Procaine Penicillin G 50,000 U/kg/day IM for 10days If >1 day of therapy missed, entire course should be restarted!
Treatment Asymptomatic, Normal CSF exam, CBC, platelets, and Radiologic exam: 1. No maternal tx aqueous PCN G IV for 10-14 days 2. Tx w/ Erythromycin clinical, serologic follow-up, and Benzathine Pcn G IM x 1 3. Tx < 1month before Delivery, or <4 fold Decrease in titers clinical, serologic follow-up and Benzathine Pcn G IM x 1
Treatment • Treat all newborns w/ positive VDRL as if they have congenital syphilis, even if mother thought to not have an active infection. • Difficult to document that mother received adequate tx, and has falling VDRL titer. 2. Low titer VDRL test may be compatible with latent maternal syphilis. 3. Newborn may not have clinical manifestations at birth. 4. Compliance with follow-up visits may be problem.
Follow-up • Should have careful follow-up examination at • 1, 2, 4, 6, and 12 months of age. • Serologic non-treponemal tests: 3, 6, 12 months, and end of tx • (or until non-reactive) • Non-treponemal Ab titers decline by 3 months of age, and • Should be Non-reactive by 6 months, if infant was not infected. • (transplacentally aquired antibodies.) • If persistent, stable titers, consider retreatment. • Congenital neurosyphilis- CSF exam at 6 month intervals until normal
Research Advances • UT Southwestern Medical Center at Dallas research team has • develop 2 blood test that quickly and reliably diagnose • Congenital syphilis in newborns. (June, 2002) • Detect neonatal antibodies to the syphilis bacterium or the • DNA of the syphilis organism itself, as predictors of CNS • Invasion. (one day vs. ten days of PCN) • IgM Immunoblotting test 2. PCR • In 1998 scientist at UTHSC in Houston, Institute for Genomic • Research in Maryland, mapped the 1.1 million base pairs of DNA that • make up the syphilis genome.Entire genomic pattern of Treponema • Pallidum now known. Difficult to study previously b/c of • dependence on mamalian host for viability. New breakthroughs?