Exercise Management
Exercise Management. Myocardial Infarction Chapter 06. Pathophysiology Coronary Atherosclerosis Significant Plaque Occlusion Ischemic Events Thrombosis, and Infarction. Coronary Thrombosis. Exercise Management - Myocardial Infarction. Exercise Management - Myocardial Infarction.

Exercise Management
E N D
Presentation Transcript
Exercise Management Myocardial Infarction Chapter 06
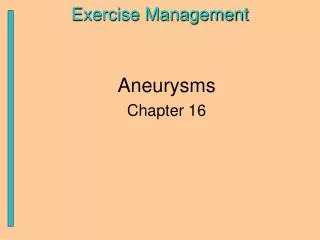
Pathophysiology Coronary Atherosclerosis Significant Plaque Occlusion Ischemic Events Thrombosis, and Infarction Coronary Thrombosis Exercise Management - Myocardial Infarction
Exercise Management - Myocardial Infarction • Myocardial Infarction (MI) Signs /Symptoms • Severe chest pain / pressure radiating to arms, back, or neck. Frequently associated with sweating, nausea, and vomiting • Dead (necrotic) myocardial muscle cells secret CPK (creatinephosphokinase) and elevate blood levels of CPK. Trace amounts of troponin may also be present. • ECG changes (ST segment elevation, T wave inversion) in the leads that detect the region of the infarction. ST Segment Elevation
Exercise Management - Myocardial Infarction • Basic types of MI’s • Transmural – extends the full thickness of the ventricular wall • Subendocardial – limited to the inner layer of the ventricular myocardium
Exercise Management - Myocardial Infarction • MI’s are described according to the involvement of the coronary circulation: • Anterior (Wall) • Posterior (Wall) • Septal • Lateral • Or larger area combinations • Anterolateral • Anteroseptal
Exercise Management - Myocardial Infarction • Cardiovascular Morbidity and Mortality is largely determined by: • The extent of Left Ventricular (LV) damage and dysfunction. Criterion measure is LV ejection fraction. • Degree of resultant myocardial ischemia, which suggests future problems with myocardial vitality • Level of Cardiorespiratory Fitness (METS) where increase risk of 5-year motality when capacity in < 4 METS
Exercise Management - Myocardial Infarction • MI Effects on the Exercise Response • ↓ Contractility = ↓ Cardiac Output = ↓O2 delivery • ↓ SBP response to exercise load resulting in exertional hypotension • ↑ ischemia, ↑angina, ↑ventricular arrhythmias • Subnormal aerobic exercise capacity (50-70%) • Chronotropic impairment may occur with damabe to the SA or AV node. This blunting or HR will reduce Cardiac Output.
Exercise Management - Myocardial Infarction • Effects of Exercise Training • ↑ Max Vo2(mean 20%) which generally rises inversely with pre-training value • ↑ in the ventilatory response to exercise • ↑ HR variability ( adjusting to workloads) • ↑ HDL-C • ↑ Psychosocial well being and self-efficacy • Relief of angina symptoms due to ↓ in myocardial oxygen demand at any given submax. work rate
Exercise Management - Myocardial Infarction • Effects of Exercise Training • Typical reductions in body mass, fat, cholesterol, and blood pressure. • ↓ coronary inflammatory markers. • ↓ blood platelet adhesiveness, fibrinogen, and blood viscosity and increased fibrinolysis. • ↑ numbers of endothelial progenitor cells and circulating angiogenic cells – promotion of endothelial repair and growth. • ↑ vagal tone and ↓ adrenergic activity
Exercise Management - Myocardial Infarction • Note - Patients who have BOTH left ventricular dysfunction and exercise induced myocardial ischemia show little or no increase in VO2 max after early outpatient rehabilitation. • Thus, success of exercise training does depend on the degree of ventricular damage and oxygen delivery capacity to the myocardium • Types of patients include those with MI to a large portion of the anterior wall and those with silent ischemia (↓ O2 delivery).
Exercise Management - Myocardial Infarction • Management and Medications • Minimize the severity of the clinical symptoms resulting from the MI • Attempt to slow, halt, or reverse the progression of atherosclerosis through medication and health behavior management (diet, exercise, stress management) • Additional surgical intervention may be required to increase blood flow to high risk areas of the myocardium (bypass, angioplasty)
Exercise Management - Myocardial Infarction • Medications • Effects of various medications used to control the risk factors associated with MI should be considered. • What effect does the medication have on exercise performance? • HR ? (chronotropic vs. ionotropic effects) • Contractility? • SBP ? • Circulating Ions used on muscle contractions (K) • Overall “feeling” of the patient • You do not need to memorize the effects of drugs. You should always review medications (See Appendix A , pp.403-06)
Exercise Management - Myocardial Infarction • Recommendations for Exercise Testing • See pg. 54 text (Table 6.1) for summary chart • Should begin with low-level testing < 5 METS • Test will serve to assess: • Functional capacity • Diagnosis of hemodynamic compromise • Prognosis ( predictor of disease progression) • Future exercise therapy ( exercise capacity and progression) • Test can improve patient confidence
Exercise Management - Myocardial Infarction • Abnormal Exercise Test Findings: • Angina / Low functional capacity ( < 4 METS) • Ischemic changes on ECG (ST segment depression) at < 4 METS. • Low Double Product • Exertional Hypotension • These findings indicate additional areas of the myocardium that may be in jeopardy • Thus, the exercise test will be symptom limited until peak performance is attained. • LVH, LBBB, pacemaker rhythms and digitalis can alter ST-segment changes so perfusion testing is indicated to detect ischemia in these conditions.
Exercise Management - Myocardial Infarction • Primary Objectives for Exercise Testing • Determine the chronotropic capacity and HR recovery • Determine aerobic (functional) capacity • Myocardial aerobic capacity ( measured by Peak Double Product [ a.k.a. rate-pressure product] (HR X SBP) • Exertional symptoms (angina, pre-syncope, syncope, ataxia) • Associated changes in the electrical conductivity function of the heart (arrhythmias, ST-T wave changes)
Exercise Management - Myocardial Infarction • Indicators of Poor Prognosis from Exercise Testing • Ischemic ST-segment depression at a low level of exercise stress • Low functional capacity (< 4 METS) • Low double product • Hypotensive (low SBP) response to an increasing exercise load.
Exercise Management - Myocardial Infarction Recommendations for Outpatient Exercise Programming (see charts p. 55) • Intensity between 40-80% VO2 max, RPE 11-16 / 20 (Borg Scale) especially for those patients on meds that effect HR. • Frequency 4-7 days/week • Duration 20-40 minutes/session continuous or accumulated • Mode – useful in ADL’s, use large muscle groups, and rhythmical. • 5-10 min warm-up and cool down (monitor medicated individuals for post-ex. hypotension)
Exercise Management - Myocardial Infarction End of Presentation