Download
1 / 69
730 likes | 1.08k Views
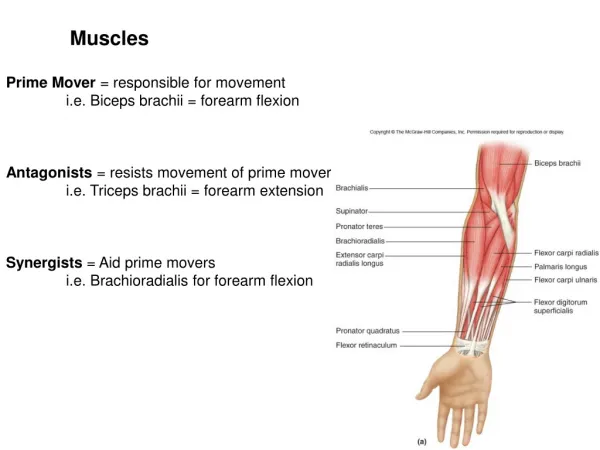
DISEASES OF MUSCLES. Symptoms of diseases of Muscle. Symptoms of diseases of muscle can be as follows: Muscular weakness Spasticity/rigidity Loss of muscular control Myoclonus Myalgia (muscular pain). Diagnostic procedures that may reveal muscular disorders include:

E N D
DISEASES OF MUSCLES Dr. Alka Stoelinga
Symptoms of diseases of Muscle Symptoms of diseases of muscle can be as follows: • Muscular weakness • Spasticity/rigidity • Loss of muscular control • Myoclonus • Myalgia (muscular pain). Diagnostic procedures that may reveal muscular disorders include: • Direct clinical observations • The testing of various chemical and antigen levels in the blood, and • Electromyography (EMG)Measuring electrical activity in muscles. • Muscle biopsy • Diagnostic imaging may be helpful in certain cases, like strokes or tumors. Dr. Alka Stoelinga
Polymyositis • Polymyositis is a type of chronic inflammatory myopathy related to dermatomyositis and inclusion body myositis. • Polymyositis means 'many muscle inflammation' Dr. Alka Stoelinga
Presentation • Polymyositis tends to become evident in adulthood, presenting with • bilateral proximal muscle weakness often noted in the upper legs due to early fatigue while walking. • Sometimes the weakness presents itself as an inability to rise from a seated position without help or an inability to raise one's arms above one's head. • The weakness is generally progressive, accompanied by lymphocytic inflammation (mainly cytotoxic T lymphocytes). • Polymyositis, strikes females with greater frequency than males. • The skin involvement is absent in Polymyositis. • Interstitial lung disease. • Investigations to detect interstitial lung disease should be performed during the initial evaluation as well as during follow-up of patients with myositis, because • ILD is a frequent manifestation in patients with Polymyositis or dermatomyositis • ILD is associated with increased morbidity and mortality. • This evaluation should include • Chest radiograph • CT of lungs • Pulmonary function tests including diffusing capacity, and • Serum levels of anti-Jo1 antibodies. Dr. Alka Stoelinga
Causes • The cause is unknown but related to autoimmune factors, genetics, and perhaps viruses. • In rare cases, the cause is known to be infectious, associated with the pathogens that cause Lyme disease, toxoplasmosis. • It is hypothesized that an initial injury causes release of muscle auto antigen, which is • subsequently taken up by macrophages and presented to CD4+ TH cells. • Activated TH cells synthesize IFN-γ that stimulate further macrophages and further inflammatory mediator release like IL-1 and TNF-α • Another important event in the pathogenesis of Polymyositis is the increased expression of MHC proteins. • Auto-Ag is presented in association with MHC-I molecules on the surface of Myocytes and is recognized by CD8 cytotoxic T cells that subsequently initiate m/s destruction Dr. Alka Stoelinga
Diagnosis • Diagnosis is fourfold, including • Elevation of creatine kinase • History and physical examination • Electromyograph (EMG) alteration • A positive muscle biopsy. • Sporadic inclusion body myositis (sIBM): IBM is often confused with polymyositis and dermatomyositis- that does not respond to treatment is likely IBM. • sIBM comes on over months to years, polymyositis comes on over weeks to months. • It appears that sIBM and polymyositis share some common features, especially the initial sequence of immune system activation, however, polymyositis does not display the subsequent muscle degeneration and protein abnormalities as seen in IBM. • Polymyositis tends to respond well to treatments, IBM does not. Dr. Alka Stoelinga
Symptoms • Symptoms include • Pain, with marked weakness and/or loss of muscle mass in the proximal musculature, particularly in the shoulder and pelvic girdle. • The hip extensors are often severely affected, leading to particular difficulty in ascending stairs and rising from a seated position. • Thickening of the skin on the fingers and hands (sclerodactyly) is a frequent feature, although this is non-specific and occurs in other autoimmune connective tissue disorders. • Dysphagia (difficulty swallowing) and/or other aspects of oesophageal dysmotility occur in as many as 1/3 of patients. • Low grade fever and peripheral adenopathy may be present. • Foot drop in one or both feet can be a symptom of advanced Polymyositis(PM) • and inclusion body myositis. • Associated with interstitial lung diseases. • Polymyositis is linked to an increase in the occurrence of certain cancers, particularly ovarian, lung, pancreatic, stomach, and colorectal cancers Dr. Alka Stoelinga
Laboratory findings • Presence of Anti Jo antibodies in >65% of patients. • Elevated serum creatine kinase is characteristic, but not specific to Polymyositis. Dr. Alka Stoelinga
Treatment • Typically, high-dose steroids are the treatment of choice. • Generally, muscle strength will improve within 4-6 weeks (useful to distinguish from inclusion body myositis). • Unresponsive patients may be tried other immunosuppressive medications. • IVIG has also shown to be a beneficial treatment. • Specialized exercise therapy may supplement treatment to enhance quality of life. Dr. Alka Stoelinga
Dermatomyositis • Dermatomyositis (DM) is a connective-tissue disease related to Polymyositis (PM) that is characterized by inflammation of the muscles and the skin Dr. Alka Stoelinga
Causes • The cause is unknown, but it may result from either a viral infection or an autoimmune reaction. • In the latter case it is a systemic autoimmune disease. • Many people diagnosed with dermatomyositis were previously diagnosed with infectious mononucleosis and Epstein-Barr virus. • Triggered by the use of various statin drugs used to control blood cholesterol • A paraneoplastic phenomenon, indicating the presence of cancer • Some cases of dermatomyositis actually "overlap" (are combined with) other autoimmune diseases such as: Sjögren's syndrome, lupus, scleroderma, or vasculitis Dr. Alka Stoelinga
Signs and symptoms • The main symptoms include • Skin rash • Symmetric proximal muscle weakness which may be accompanied by pain. • The pain may resemble the type experienced after strenuous exercise. • Some dermatomyositis patients have little pain, while in others (esp. in JDM), the pain may be severe. • Muscle may deteriorate and render the infected temporarily paralyzed unable to walk, run, get out of bed, or even swallow food and liquids. • Skin findings occur in dermatomyositis but not PM • Are generally present at diagnosis. • Gottron's signis an erythematous, scaly eruption occurring in symmetric fashion over the MCP and interphalangeal joints (can mimic psoriasis). • The heliotrope or "lilac" rash is a violaceous eruption on the upper eyelids and in rare cases on the lower eyelids as well, often with itching and swelling (most specific, though uncommon) Dr. Alka Stoelinga
Signs and symptoms • Shawl (or V-) sign is a diffuse, flat, erythematous lesion over the back and shoulders or in a "V" over the posterior neck and back or neck and upper chest, worsens with UV light. • Erythroderma is not a flat, erythematous lesion similar to the shawl sign but located in other areas, such as the malar region and the forehead. • Periungual telangiectasias and erythema. • Mechanic's hands (also in PM) refers to rough, cracked skin at the tips and lateral aspects of the fingers forming irregular dirty-appearing lines that resemble those seen in a laborer (this is also associated with the anti-synthetase syndrome) • Psoriaform changes in the scalp • Centripetal flagellate erythema comprises linear, violaceous streaks on the trunk (possibly caused by itching pruritic skin) • Calcinosis cutis (deposition of calcium in the skin) is usually seen in juvenile dermatomyositis, not adult dermatomyositis. • Dysphagia (difficulty swallowing) is another feature, occurring in as many as 33% of cases. Dr. Alka Stoelinga
Diagnosis • The diagnosis of dermatomyositis can be confirmed by • Muscle biopsy • EMG • Blood tests • Only muscle biopsy is truly diagnostic (pathognomic) • Liver enzymes and EMG are relatively non-specific • Creatine Phosphokinase (CPK), are the major tool in assessing the progress of the disease and/or the efficacy of treatment. • Muscle biopsy shows two classic microscopic findings in dermatomyositis: • A mixed B- and T-cell perivascular inflammatory infiltrate • Perifascicular muscle fiber atrophy • Dermatomyositis is associated with autoantibodies, especially anti-Jo1 antibody. Dr. Alka Stoelinga
Treatment • This disease has no known cure • Specialized exercise therapy may supplement treatment to enhance quality of life. • Medications to help relieve symptoms include: • Prednisolone • Methotrexate • Mycophenolate • Intravenous immunoglobulin • Azathioprine • Cyclophosphamide • Rituximab Dr. Alka Stoelinga
MUSCULAR DYSTROPHY • Muscular dystrophy (MD) refers to a group of hereditary muscle diseases that weaken the muscles that move the human body. • Muscular dystrophies are characterized by progressive degeneration of a group of muscles without involvement of the nervous system. • Defects in muscle proteins, and the death of muscle cells and tissue. Classification • Duchenne Muscular Dystrophy • Becker’s Muscular Dystrophy • Limb girdle Muscular Dystrophy • Congenital Muscular Dystrophy • Facioscapulohumeral Muscular Dystrophy • Myotonic Muscular Dystrophy • Oculopharyngeal Muscular Dystrophy • Distal Muscular Dystrophy • Emery- Dreifuss Muscular Dystrophy • There are more than 100 diseases in total with similarities to muscular dystrophy. • Most types of MD are multi-system disorders with manifestations in body systems including the heart, gastrointestinal and nervous systems, endocrine glands, skin, eyes and other organs. Dr. Alka Stoelinga
Clinical features: • Predominantly proximal muscle involvement • Symmetrical wasting and weakness • Deep Tendon reflexes are preserved until late stage. • Atrophy and pseudohypertrophy • No sensory/Autonomic/Bladder/CNS symptoms Dr. Alka Stoelinga
Main symptoms include: • Progressive muscular wasting • Poor balance • Frequent falls • Walking difficulty • Waddling gait • Calf deformation • Limited range of movement • Respiratory difficulty • Drooping eyelids • Loss of bladder control • Scoliosis (curvature of the spine and the back) • Inability to walk • Few or none of these symptoms may be present before diagnosis. Some types of muscular dystrophy can affect the heart, causing cardiomyopathy or arrhythmias. Dr. Alka Stoelinga
Investigation: • Electromyography(EMG) • Muscle biopsy • Serum Creatinine Phosphokinase (CPK MM/ 3) is markedly Raised in Duchenne muscular dystrophy but normal or moderately raised in other types Management: • No specific therapy • Physiotherapy is helpful Dr. Alka Stoelinga
1. DUCHENNE MUSCULAR DYSTROPHY • Duchenne muscular dystrophy (DMD) is a severe recessive X-linked form of muscular dystrophy characterized by: • Rapid progression of muscle degeneration, eventually leading to loss of ambulation and death. • (DMD) is the most common childhood form of muscular dystrophy, becoming clinically evident when a child begins walking. Patients typically require a wheelchair by age 10 to 12 and die in their late teens to early 30s, though some people with Duchenne muscular dystrophy are now living to age 40 and beyond. • Occurs one in 3500 males, making it the most prevalent of muscular dystrophies. • In general, only males are affected, though females can be carriers. Dr. Alka Stoelinga
The disorder is caused by a mutation in the gene DMD, located in humans on the X chromosome (Xp21). • The DMD gene codes for the protein dystrophin, an important structural component within muscle tissue. • Dystrophin is part of a complex structure involving several other protein components. • The "dystrophin-glycoprotein complex" helps anchor the structural skeleton (cytoskeleton) within the muscle cells, through the outer membrane (sarcolemma) of each cell, to the tissue framework (extracellular matrix) that surrounds each cell. • Due to defects in this assembly, contraction of the muscle leads to disruption of the outer membrane of the muscle cells and eventual weakening and wasting of the muscle Dr. Alka Stoelinga
Clinical features: • Symptoms usually appear in male children before age 6 and may be visible in early infancy. • Progressive proximal muscle weakness of the legs and pelvis associated with a loss of muscle mass is observed first. • Eventually this weakness spreads to the arms, neck, and other areas. • Early signs may include pseudohypertrophy (enlargement of calf muscles), difficulties in standing unaided or inability to ascend staircases, frequent fall. • GOWER’s sign • As the condition progresses, muscle tissue experiences wasting and is eventually replaced by fat and fibrotic tissue (fibrosis)Joint contracture. • By age 10, braces may be required to aid in walking but most patients are wheelchair dependent by age 12. Dr. Alka Stoelinga
Later symptoms may include abnormal bone development that lead to skeletal deformities, including curvature of the spine. • Due to progressive deterioration of muscle, loss of movement occurs eventually leading to paralysis. • Intellectual impairment may or may not be present but if present, does not progressively worsen as the child ages. • Recurrent pulmonary infection • Development of Cardiomyopathy • The average life expectancy for patients affected with DMD varies from early teens to age mid 30s. • There have been reports of DMD patients surviving past the age of 40 and even 50. Dr. Alka Stoelinga
Investigations: • CPK: Markedly raised(100-200 times) • EMG: Shows myopathic pattern • Muscle biopsy: Shows fiber necrosis, Regeneration and replacement by fat. Dr. Alka Stoelinga
Treatment • There is no known cure for Duchenne muscular dystrophy, although recent stem-cell research is showing promising results that may replace damaged muscle tissue. Treatment is generally aimed at controlling the onset of symptoms to maximize the quality of life, and include the following. • Corticosteroids such as prednisolone and deflazacort increase energy and strength and defer severity of some symptoms. • Mild, non-jarring physical activity such as swimming is encouraged. Inactivity (such as bed rest) can worsen the muscle disease. • Physical therapy is helpful to maintain muscle strength, flexibility, and function. • Orthopedic appliances (such as braces and wheelchairs) may improve mobility and the ability for self-care. Form-fitting removable leg braces that hold the ankle in place during sleep can defer the onset of contractures. • Appropriate respiratory support as the disease progresses is important Dr. Alka Stoelinga
Prognosis • Duchenne muscular dystrophy eventually affects all voluntary muscles and involves the heart and breathing muscles in later stages. • The life expectancy typically ranges from the late teens to the mid-30s. • However, some people with Duchenne muscular dystrophy are now living to age 40 and beyond. • Recent advancements in medicine are extending the lives of those afflicted. Dr. Alka Stoelinga
Physical Therapy • Physical therapists are concerned with enabling children to reach their maximum physical potential. Aim is to: • Minimize the development of contractures and deformity by developing a program of stretches and exercises where appropriate • Anticipate and minimize other secondary complications of a physical nature • Monitor respiratory function and advice on techniques to assist with breathing exercises and methods of clearing secretions • Schedule weekly to monthly sessions at a massage therapist to decrease the present pain. Dr. Alka Stoelinga
Becker's muscular dystrophy 2. Becker's muscular dystrophyis an X-linked recessive inherited disorder characterized by slowly progressive muscle weakness of the legs and pelvis • BMD is caused by the production of a truncated, but partially functional form of dystrophin , resulting in instability in the structure of muscle cell membrane. • Survival is usually into old age • Becker's muscular dystrophy is related to Duchenne muscular dystrophy in that both result from a mutation in the dystrophin gene, but in Duchenne muscular dystrophy no functional dystrophin is produced making DMD much more severe than BMD. • Both Duchenne and Becker's muscular dystrophy have traditionally been called "X-linked" recessive diseases. Dr. Alka Stoelinga
Clinical features: • Muscle weakness , slowly progressive (Difficulty running, hopping, jumping; Progressive difficulty walking) • Toe-walking (walking on toes; also known as equinus) • Use of Gower's Maneuver to get up from floor. • Frequent falls • Difficulty in breathing • Non progressive cognitive dysfunction only in rare cases: not as common as in Duchenne Muscular Dystrophy because the brain only needs small amounts of dystrophin. • Calf muscle enlargement (pseudohypertrophy) is quite obvious. • Cardiomyopathy may occur, but the development of congestive heart failure or arrhythmias (irregular heartbeats) is rare. • Loss of ambulation (loss of ability to walk) may not occur until the person is in his fifties. Dr. Alka Stoelinga
INVESTIGATION • Creatine kinase (CPK) levels may be elevated. • An electromyography (EMG) shows that weakness is caused by destruction of muscle tissue rather than by damage to nerves. • Genetic testing • A muscle biopsy (immunohistochemistry or immunoblotting) or genetic test (blood test) confirms the diagnosis. Dr. Alka Stoelinga
Treatment: • There is no known cure for Becker's muscular dystrophy. • Treatment is aimed at control of symptoms to maximize the quality of life. • Activity is encouraged. • Inactivity (such as bed rest) or sitting down for too long on plane or car rides can worsen the muscle disease. • Physical therapy may be helpful to maintain muscle strength. • Orthopedic appliances such as braces and wheelchairs may improve mobility and self-care. • Genetic counseling may be advisable when potential carriers or patients want to have children. • Sons of a man with Becker's muscular dystrophy do not develop the disorder, but daughters will be carriers (and some carriers can experience some symptoms of muscular dystrophy). The daughters' sons may develop the disorder. • Immunosuppressant steroids like Prednisone have been known to help slow the progression of Becker Muscular Dystrophy. Dr. Alka Stoelinga
Prognosis: • Becker's muscular dystrophy results in slowly progressive disability, and patients eventually use a cane or wheelchair. • Death can occur from age 40 but some patients enjoy a nearly normal lifespan. Dr. Alka Stoelinga
Complications • Deformities • Permanent, progressive disability manifested as decreased mobility • Mental impairment - However, this is much less common than DMD. • Cardiomyopathy • Pneumonia or other respiratory infections • Respiratory failure Dr. Alka Stoelinga
3.LIMB GIRDLE MUSCULAR DYSTROPHY • Limb-girdle muscular dystrophy or Erb's muscular dystrophy is an Autosomalclass of muscular dystrophy that is similar but distinct from Duchenne muscular dystrophy and Becker’s muscular dystrophy. • Limb-girdle muscular dystrophy encompasses a large number of rare disorders Dr. Alka Stoelinga
The term "limb-girdle" is used to describe these disorders because the muscles most severely affected are generally those of the hips and shoulders -- the limb girdle muscles. • Common symptoms of limb-girdle muscular dystrophy are: • Muscle weakness • Myoglobinuria • Myotonia • Cardiomyopathy • Elevated serum CK • The muscle weakness is generally symmetric, proximal, and slowly progressive. Dr. Alka Stoelinga
Generally pain is not present with LGMD, and mental function is not affected. • LGMD can begin in childhood, adolescence, young adulthood or even later. • The age of onset is usually between 10 and 30. • Both genders are affected equally. • When limb-girdle muscular dystrophy begins in childhood the progression appears to be faster and the disease more disabling. • When the disorder begins in adolescence or adulthood the disease is generally not as severe and progresses more slowly. Dr. Alka Stoelinga
Treatment • Treatment for LGMD is primarily supportive. • Exercise and physical therapy are advised to maintain as much muscle strength and joint flexibility as possible. • Calipers may be used to maintain mobility and quality of life. • Careful attention to lung and heart health is also required. • IV Ig may increase strength in some forms and prevent progression in others • Corticosteroids : Helps to Prevent fibrosis and inflammation without the secondary weakening . Dr. Alka Stoelinga
Prognosis: • The person with LGMD loses muscle bulk and strength. • Eventually, patient may need a power wheelchair or scooter, especially for long distances. • While LGMD isn't a fatal disease, it may eventually weaken the heart and lung muscles, leading to illness or death due to secondary disorders Dr. Alka Stoelinga
4.CONGENITAL MYOPATHY • Congenital myopathy refers to a group of muscle disorders that appear at birth or in infancy. • Typically, an infant with a congenital myopathy will be "floppy," have difficulty breathing or feeding, and will lag behind other babies in meeting normal developmental milestones such as turning over or sitting up. • Muscle weakness can occur for many reasons, including a problem with nerve that stimulates the muscle/ brain. • Muscle degeneration may be mild or severe. • Problems may be restricted to skeletal muscle, or muscle degeneration may be paired with effects on the brain and other organ systems. • A number of the forms of the congenital muscular dystrophies are caused by defects in proteins that are thought to have some relationship to the dystrophin-glycoprotein complex and to the connections between muscle cells and their surrounding cellular structure. • Some forms of congenital muscular dystrophy show severe brain malformations, such as lissencephaly and hydrocephalus • Therefore, to diagnose a congenital myopathy, a neurologist will perform a detailed physical exam as well as tests to determine the cause of weakness. INVESTIGATIONS: • Creatinine kinase • EMG • Muscle biopsy, and • Genetic testing. Dr. Alka Stoelinga
5.Facioscapulohumeral muscular dystrophy • Facioscapulohumeral muscular dystrophy is an AD form of muscular dystrophy that initially affects the skeletal muscles of the face (facio), scapula (scapulo) and upper arms (humeral). • Symptoms may develop in early childhood and are usually noticeable in the teenage years with 95% of affected individuals manifesting disease by age 20 years. • A progressive skeletal muscle weakness usually develops in other areas of the body as well • The weakness is asymmetrical. • Life expectancy is normal, but up to 15% of affected individuals become severely disabled and eventually must use a wheel chair • Non-muscular symptoms frequently associated with FSHD include subclinical sensorineural hearing loss and retinal telengectasia. Dr. Alka Stoelinga
CLINICAL FEATURES • Facial muscle weakness (eyelid drooping, inability to whistle, decreased facial expression, depressed or angry facial expression, difficulty pronouncing the letters M, B, and P) • Shoulder weakness (difficulty working with the arms raised, sloping shoulder) • Hearing loss • Abnormal heart rhythm • Unequal weakening of the biceps, triceps, deltoids, and lower arm muscles • Loss of strength in stomach muscles and eventual progression to the legs • Foot drop Dr. Alka Stoelinga
6.MYOTONIC MUSCULAR DYSTROPHY • Myotonic dystrophy (dystrophia myotonica) is Chronic, slowly progressing, highly variable inherited multisystemic disease that can manifest at any age from birth to old age. • It is characterized by : • Wasting of the muscles • Posterior subcapsular cataracts • Heart conduction defects • Endocrine changes and • Myotonia (difficulty relaxing a muscle). • The highly variable age of onset decreases with successive generations. • Thus the disease shows at an earlier age in successive generations a phenomenon termed anticipation. Dr. Alka Stoelinga