Download
1 / 22
410 likes | 1.33k Views
The Consultation – Models, Tasks, Skills. Dr Elke Hausmann GP ST1 GP group 28/09/2011. Interest in the consultation. There is more to the consultation than a patient presenting with a medical problem for the doctor to solve

E N D
The Consultation – Models, Tasks, Skills Dr Elke Hausmann GP ST1 GP group 28/09/2011
Interest in the consultation • There is more to the consultation than a patient presenting with a medical problem for the doctor to solve • Both Dr and patient are individuals in particular contexts (family, community, society) – problem may or may not be medical • Psychologists, psychoanalysts, social scientists, philosophers, doctors…
Interest in the consultation • What does happen? (empirical research) • What should happen? (the ‘ideal consultation’, based on particular values – or what gives results, based on empirical work) • What could happen? (not all consultations are the same – different tasks) • Skills – allow the Dr to achieve a good consultation
Balint 1957Trained doctor and psychoanalyst – worked with GP groups ‘The doctor, his patient and the illness’ • Nearly all problems presenting to the Dr have a psychological element to them • Doctors have feelings and feelings have a function in the consultation • Explore psychological/emotional aspects of consultation and use insight for benefit of the patient • The doctor as drug – the doctor has a therapeutic role in all consultations, not only those with a defined disease process
Berne 1958Psychiatrist – ‘games people play’ • Transactional analysis • Model of the human psyche: three ‘ego states’ • Critical or Caring Parent – commands, directs, prohibits, controls, nurtures • Logical Adult – sorts out info and works logically • Spontaneous or Dependent Child – intuition, creativity, spontaneity, enjoyment • Parent-doctor and child-like patient? TA approach to increase doctor’s repertoire, break out of repetitious cycles of behaviour (‘games’)
RCGP triaxial model 1972RCGP working party’s ‘job description’ of the GP • ‘The Future General Practitioner’ • Consideration of the physical, psychological and social condition of the patient • Not to think purely in terms of organic illness
Heron 1975Humanist psychologist – approach now used in business, education, public service etc Six Category Intervention Analysis (3 doctor- and 3 patient-centred – authoritative and facilitative categories) • Prescriptive – giving explicit advice or instructions • Informative – imparting new knowledge (relevant to patient? Enough? Not enough?) • Confronting – challenging a restrictive attitude or behaviour, may cause upset – needs follow up! • Cathartic – seeking to release emotion (weeping, laughter, trembling, anger) to move forward • Catalytic – encouraging the pat to discover and explore his own latent thoughts and feelings • Supportive – offering comfort and approval, affirming the pat’s intrinsic value – allow patient to cope better
Becker and Maiman 1975Developed from Rosenstock 1966 for studying and promoting the uptake of health services (TB) Health Belief Model – decision to consult depends on: • Health motivation - The individual’s general interest in health matters, acc to personality, soc class, ethnic group etc • Perceived vulnerability and perceived seriousness - How vulnerable or threatened a pat feels to be by a particular disease • Perceived cost/benefits of an action - The individual’s estimation of the beliefs of treatment weighed against cost, risks and inconvenience • Cues to action - Trigger factors, such as alarming symptoms, advice from family or friends, messages from the mass media, disruption of work and play
Health Belief Model Patients vary enormously in the way they accept responsibility for their health (locus of control) • Internal controller – patients who feel they control their own health destiny, have firm idea of own diagnosis and expectations of what Dr should do for them • External controller – patients feel their likelihood of developing illness or staying healthy is completely out of their control, modifying lifestyle does not make a difference • Powerful other – patients who feel their health destiny rests with a particular person (could be GP), respond to their advice
Byrne Founder member RCGP + Long Psychologist 1976Based on 2500 tape-recorded consultations from over 100 Drs in UK and NZ • ‘Doctors talking to patients’ – doctor-centred • Style of consultation depends on personality of doctor and patient – doctor-dominated to virtual monologue by patient • Narrow repertoire of consultations skills – doctors who ask more open questions see their patients less frequently • 6 stages to consultation (establish relationship, discover reason for attendance, history +/-examination, dr + pat consider condition (illness), discussion of Rx or further Ix, closingconsultation)
Stott and Davies 1979Academic GPs 4 tasks that can take place in each consultation: • Managing the presenting complaint (eg sore throat) • Modifying health-seeking behaviour (eg self-medication for future episode in pat presenting repeatedly in 24 hrs for sore throat) • Managing ongoing problems (eg DM, depression) • Opportunistic health promotion (eg smoking, weight, cervical smear, immunisation…)
Helman 1981GP and medical anthropologist – ‘Suburban Shaman’ 2006 Folk Model of Illness – illness vs disease • what has happened? • why? • why me? • why now? • what would happen if nothing were done? • what should be done about it?
Pendleton 1984Social psychologist – PhD on analysis of the consultation The doctor’s tasks - seven tasks model • Define reason for attendance (ICE, effects of illness = patient’s agenda) • Consider other problems • Doctor and patient choose appropriate action • Share understanding with patient • Involve patient in management decisions • Use time (new) and resources well • Establish and maintain dr-pat relationship
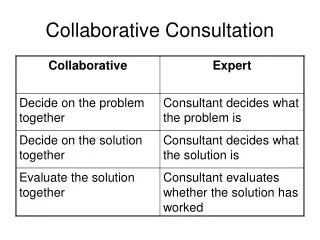
Tuckett et al 1985Medical sociology – study of doctor-patient communication in GP ‘Meeting between experts’ • Consultation as meeting between two experts • Doctor expert in medicine (underlying pathology, differential diagnosis) • Patient expert in own illnesses (unique illness experience) • Shared understanding is the aim • Doctors should seek to understand the patient’s beliefs • Doctors should address explanations in terms of the patient’s belief system Example: patient repeatedly comes in with chest pain, re-assured it’s not cardiac – turns out his uncle recently died of cancer of the oesophagus
Neighbour 1987Former RCGP president ‘The Inner Consultation’ – the doctor’s two heads: organiser and responder (while being active organiser it’s difficult being responsive and vice versa) 5 checkpoints: • Connecting – develop rapport/empathy • Summarising – reasons for attending, feelings, concerns, expectations • Handing over – sharing agreed mx plan, hands control back to pat • Safety-netting - making contingency plans • Housekeeping – getting ready for next pat (new: safe doctoring and healthy doctor!)
Fraser 1992Professor of GP in Leicester – ‘Clinical method – a General Practice approach’ Areas of competence: • Interviewing and history taking • Physical examination • Diagnosis and problem-solving – current probability about cause of illness rather than certainty • Patient management (RAPRIOP – reassurance/explanation, advice/counselling, prescribing, referral, investigations, observation + follow-up, prevention) • Relating to patients – friendly but professional • Anticipatory care – health promotion/disease prevention • Record-keeping
Tate 1994Developed from Pendleton – retired GP and former Convenor of MRCGP examinations ‘The Doctor’s Communication Handbook’ • Importance of ideas, concerns, expectations • Updates strategies and skills in internet-era
Stewart and Roter 1997American academics (John Hopkins University) – research using audiotapes Gathering of info about patient’s problems along two parallel pathways • Patient’s agenda – exploring ideas, concerns, expectations, feelings, thoughts and effects culminating in an understanding of the patient’s unique experience of the illness • Doctor’s agenda – exploring symptoms, signs, investigations and consideration of the underlying pathology and diff diagnosis • Need to be brought together for shared understanding – allows for explanations, planning and decision-making
Calgary-Cambridge 1996Derives from Pendleton – evidence-based approach to integration of the ‘tasks’ of the consultation and improving skills for effective communication • Initiating the session (rapport, reasons for consulting, establishing shared agenda) • Gathering information (patient’s story, open and closed questions, identifying verbal and non-verbal cues) • Building the relationship (developing rapport, recording notes, accepting patients’ views/feelings and demonstrating empathy and support) • Explanation and planning (giving digestible info and explanations) • Closing the session (summarising and clarifying the agreed plan)
Launer 2002London GP ‘Narrative-based’ model of the consultation – techniques to help understanding the patient’s story: • Circular questioning or picking up patients’ words to form open questions and help patients to focus on meaning • A focus on listening (avoid note-taking during consultation) • Exploring the context of the problem (family, work, community) • Conversations circularity co-creation curiosity contexts caution
To do in the next consultationbased on e-GP learning module on the consultation • check patient's understanding • try to see from patient's perspective • modify help-seeking • ideas, concerns, expectations • cues to hidden agenda? • summarise • safety-netting • negotiate agenda
References • www.patient.co.uk/doctor/Consultation-Analysis.htm • http://www.gp-training.net/training/communication_skills/consultation/index.htm • http://www.yorksandhumberdeanery.nhs.uk/general_practice/documents/consultationmodelsindetail-BillBevington.doc • The Condensed Curriculum Guide RCGP 2007 • e-GP learning module ‘Models of the Consultation’