Download
1 / 35
350 likes | 356 Views
The Use of Non Profit, Industrial Consortia to Improve Pharmaceutical Industry R & D “Lessons Learned” Wellcome Trust’s “Pre-Competitive Boundaries and Open Innovation in Drug Discovery and Development” Meeting Arthur Holden Founder, Chairman, and CEO. Introduction. Executive not scientist

E N D
The Use of Non Profit, Industrial Consortia to Improve Pharmaceutical Industry R & D “Lessons Learned” Wellcome Trust’s “Pre-Competitive Boundaries and Open Innovation in Drug Discovery and Development” Meeting Arthur Holden Founder, Chairman, and CEO
Introduction • Executive not scientist • 30 years of leadership experience – commercial & non-profit consortia; start-ups to mid size to large corporations • Baxter International (1984-1994) • Celsis International (1994-1998) • First Genetic Trust (2000-2006) • Illumina (2006-2007) • Formed and managed numerous large-scale consortia • The SNP Consortium, Ltd. (1999-2002) • The International SAE Consortium, Ltd. (2007- 2012) • Supported many others (MSC, HapMap, etc.)
My Comments • Consortia Context • Model • TSC • SAEC • Some Lessons Learned 3
“Pharmaceuticals” Context • Declining Productivity & novel therapeutics • Increasing Costs & Competition at “Market Entry” • “Block Buster” mentality softening • Scale “Innovation” ??? • > Healthcare pricing pressures in all core markets “pay for performance” paradigm of the future • End of “biotech risk subsidy” by the public markets etc, etc, etc. Increasing R & D productivity is critical. 5
“R & D Sourcing Options” External Commercial Partnerships External Academic/Gov. Relationships In-house Operations R & D Consortia 6
Industrial Biomedical Consortium“Generic Model” Skilled External Partners Industrial Members Clear Project/ Unifying Goal(s)/ Finite Timeframe Private Foundations/ Governmental Bodies Organized by Professional Management & Supported by Quality Processes 7
Why Industrial Biomedical Consortia [IBCs]? • Fill a research gap, not being effectively filled by existing players [government or private] • Establish common/often risky “research platforms”, which help all researchers, while meeting specific industrial scientific requirements [pre-competitive/pro-competitive] • Establish industry standards • Reduce legal/IP barriers • Gain greater efficiency/effectiveness (scale) via pooling of talents and resources across industry
Two Consortia The SNP Consortium 1999-2002 The SAE Consortium 2007-2012 9
Common Characteristics (TSC/SAEC) • Defined project finite timeframe • Non-Profit [501c3] > “public benefit orientation” • Open data access • No IP constraints • “Fixed, uniform” membership contributions • Designed for “leverage” and “time to result” • Collaboration with government (if advantageous to results) • Active (Committee) Participation and Investment by Members • “Governance by majority” 1 member/1 vote 10
SNP Consortium -- Mission & Results “The SNP Consortium worked to advance the field of medicine and the development of genetic based diagnostics and therapeutics, through the creation of a high quality, dense genome wide single nucleotide polymorphism (SNP) map, which is available to all parties at no cost.” • The Results: • Created a high quality HG SNP map for GWAS • Identify 300,000 SNPs [2.7M Common SNPs] • Map 150,000 SNPs [2.5M Common SNPs] • Broad, evenly spaced well annotated map within two years • Maximize public accessibility [~ 2.4M “unencumbered” SNPs] • Provided order and orientation data to assembled base WG project sequence and a significant “backbone” to the “HapMap” • $42M project, which exceeded expectations with $9M in budget favorability 11
Drivers of the SNP Consortium • Industry standard SNP map strong industry support • Universal access to base genomic/SNP data public domain (IP considerations) • Facilitate pharmaco-genomics / genetics association, linkage & haplotyping studies • Economics: • Favorable economy of scale>>cost & risk sharing • Favorable cost to access high quality SNP datasets 12
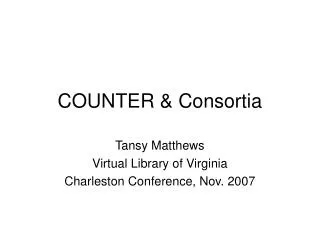
SNP@CSHL.org The SNP Consortium -DCC Summary Whitehead Sanger Wash U SNPs & Mapping Data SNPs SNPs SNPs Stanford DCC Mapping Data Reformatted SNPs & Maps Public dbSNP/EBI Consortium
iSAEC -- Mission & Results “TheiSAEC will identify and validate DNA-variants useful in predicting the risk of drug induced serious adverse events.” • The Results (to date): • Initial GWAS for Drug Induced Serious Skin Rashidentifying marker(s) of potential significance • Assembled 2nd largest DILI cohort, merged with DILIN, completed initial GWAS identifying numerous significant marker(s) within/across drugs • Initial GWAS for Drug Induced PQT/TdP, merged with LeDueq Network, and identified marker(s) of potential significance • Completed four public data releases (clinical and GWAS data) with FDA • > 200 genetic markers associated with DILI and SSR in the public domain. • Favorable to budget in phase by $2M • Organized Phase 2 focused on “drug induced immunologic SAEs” associated with specific drugs and ethnicities, and forming novel SAE research channels vital to drug-specific SAE research. 14
Drivers of the iSAEC • Need to improve new product (safety) productivity • Scale required to execute safety pharmacogenetics (top R & D management priority) common markers in public domain • Need to standardize “SAE phenotypes” • Need to develop new and innovative methods to source cases and controls • Pooled technology assessment & risk (e.g. GWAS, WG sequencing) • FDA’s Industrial Advisory Board recommendation • $ resources required (poor public funding, given the health impacts) 15
iSAEC Organization and Committees BOD Genotyping Core [Expression Analysis, Inc] Bioinformatics Core [Columbia University] CEO Scientific/Clinical SMC Legal/IP PR/ Comm. SAE [s] Data Anal. Research Collaborators [Academic & Commercial] Outsourced Service Suppliers [Legal & PR] 16
iSAEC Web Site http://www.saeconsortium.org 17
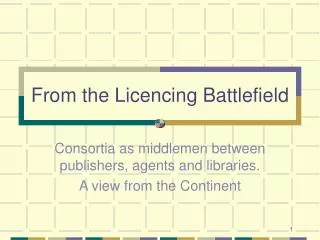
System admin Automated Data Access Assessment Data Use Agreement (Online/Hardcopy) iSAEC Data Access Process Request Form (online) Investigator Database
10 Lessons Learned (Success Factors) 1. A clear unifying objective is a must. 2. Ensure the effort is both “pre-competitive” and “pro-competitive.” 3. Have a quality “draft” operating concept/plan before recruiting members [“one shot rule”]. 4. Establish a uniform membership requirements & development strategy with potential members. 5. Establish dedicated management early in the effort /don’t reinvent the wheel. 20
10 Success Factors cont. 6. Organize well defined committees with high quality, dedicated leaders 7. Outsource…outsource… outsource to the best external advisors/ investigators via “performance based” contracts 8. Generate results that exceed expectations 9. Make it fun and say “thank you” in meaningful ways, and…. 10. Know when to fold … begin with an end in mind! 21
Learning #1 • Needed Science! • Easily Understood • Measurable • Focused vs General • All essential for member recruitment Have a Clear, Quality Objectivewhich Unifies the Membership […Full Genome Representative SNP Map… Safety related markers in the public domain] 22
Learning #2 • Pre-Competitive (moving target) • Pro-Competitive (legal anti-trust perspective) • “Public Good” orientation (Tax/Charity status) • “Neutral data access policy” “public” access to data The focus should be “pre-competitive” and “pro-competitive.” 23
Learning #3 • Well organized “formation phase” with potential members • Scientific Plan [including necessary feasibility pilots] • Informatics Plan • Legal/IP Policies • Operating Plan/Performance Metrics/Contingencies • Budget [Proactive Risk Factor Mgnt] Develop a high-quality plan [before recruiting membership] 24
Learning #4 • High Priority a Must! • Fixed Dues Structure (Annual Sensitivity [$1M down to <$.4M/year) • Do not vary membership tiers for industrial members • Non industrial members >> same $ terms for voting rights • Member Diversification has pros & cons Establish a Clear Membership Requirement & Development Strategy with potential members 25
Learning #5 • Formation phase leadership • Members are investing in both the leader/project • Defining the Organization & Key Processes • Sourcing strategies • Pre-formation negotiations • “Closing” Membership • Communication is Key • Everything takes more Effort than Planned Establish dedicated management ASAP 26
Learning #6 • SMC, Legal/IP, & Sub-committees key • Functional/Scientific Leadership is vital • Time Commitment is Greater than Expected • Senior Management Support of Manager Commitment Organize clear committees with high quality dedicated leaders 27
Learning #7 • Increases expertise & skills • Leverage existing infra-structure/investments/skill • Performance based contracts no grants! • Reduces project risk • Increases management flexibility • Careful assessment of the risks of doing the Consortium if Outsourcing is not an Option Outsource…outsource… outsource
Learning #8 • Confirms membership investment creates additional consortia opportunities • “Consortia fatigue” is real major cause is poorly managed/under performing consortia • Winning together is fun … Generate results that exceed expectations! 29
Learning #9 • Member help is essential • “Recognition starvation” is an epidemic • Everybody likes “special events” … but cost-effectiveness is vital in today’s environment Say “thank you” in meaningful ways and make the consortium a fun experience 30
Learning #10 • Finite objectives within a fixed time frame attractive to members • Consortia are strategic initiatives vs on-going concerns • New Consortia require different leadership • Effective BOD with the appropriate experience & seniority—Key! Don’t try to make a consortium into something it shouldn't be … know when to fold
Final Caveats • Wellcome Trust involvement and funding important validation to pharmcos • Involve stakeholder governmental bodies (TSC—NIH, iSAEC—FDA, EMEA, PMDA), without slowing the effort. • Limits to company leverage in these “leaner times” … funding a quality consortium is very hard these days (more freeloaders) • Vital that we learn from best efforts take these into new, important consortia efforts to improve pharma productivity 32
Acknowledgments SMC • Ann Daly & DILIGEN [Newcastle] • Mariam Molokhia & EUDRAGENE [London] • Matt Nelson [GSK] • Sally John [Pfizer] • Yufeng Shen [Columbia] • Itsik Pe’er [Columbia] • Aris Floratos [Columbia] • Mark Daly [Harvard/Broad] • David Goldstein [Duke] • Eric Lai [ex-GSK] • Donald Halbert [Abbott] • Joe Walker [D-S] • Nadine Cohen, Quingqin Serena Li, & Adrian Thomas [J&J] • Joanne Meyer & Steve Lewitzky [Novartis] • Klaus Lindpaintner & Karen Wilcock [Roche] • Steven Kovacs [Sanofi-Aventis] • Leonardo Sahelijo [Takeda] • Ted Burczynski & Maha Karnoub [Wyeth] • Robert O'Neill & Steve Wilson [FDA] • Andrea Califano [Columbia] • Allen Roses [Duke] • John Senior [FDA] Members • Brian Spear [Abbott] • Rick Scheyer [Daiichi Sankyo] • Lon Cardon [GSK] • Nadine Cohen [J&J] • Joanne Meyer [Novartis] • Aidan Power [Pfizer] • Klaus Lindpaintner [Roche] • Robert Dix [Sanofi-Aventis] • Leonardo Sahelijo [Takeda] • Michael Burczynski [Wyeth] • Janet Woodcock [FDA] • ShaAvhree Buckman [FDA] • Michael Dunn [Wellcome Trust]
Industrial ConsortiaSome Operational Tenants • Unifying objective industry and public good [501 c 3] • Focused projects, with clear objectives & strong operational management • Strong “quality” and “time to result” orientation • Clear and uniform “membership requirements” • Extensive leverage of members’ skills via well organized sub-committees • Strive to collaborate with the best quality external advisors & investigators on an international basis • Public release of data after appropriate IP management actions to ensure “openness”