Leishmaniasis
Leishmaniasis. MAJ Mark Polhemus Leishmania Treatment Center Walter Reed Army Medical Center. Introduction. Leishmaniasis is a parasitic disease transmitted by the bite of sand flies. Found in parts of at least 88 countries including the Middle East Three main forms of leishmaniasis

Leishmaniasis
E N D
Presentation Transcript
Leishmaniasis MAJ Mark Polhemus Leishmania Treatment Center Walter Reed Army Medical Center
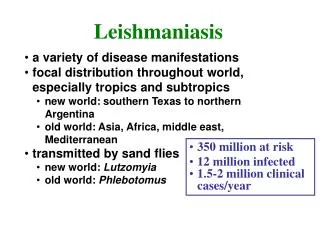
Introduction • Leishmaniasis is a parasitic disease transmitted by the bite of sand flies. • Found in parts of at least 88 countries including the Middle East • Three main forms of leishmaniasis • Cutaneous: involving the skin at the site of a sandfly bite • Visceral: involving liver, spleen, and bone marrow • Mucocutaneous: involving mucous membranes of the mouth and nose after spread from a nearby cutaneous lesion (very rare) • Different species of Leishmania cause different forms of disease
Introduction • In the Middle East L. major and L. tropica are the most common species • L. major causes skin infection • L. tropica causes skin and visceral infection and rarely causes mucocutaneous infection • About 1.5 million new cases of cutaneous leishmaniasis in the world each year • 500,000 new cases of visceral leishmaniasis estimated to occur each year also • 20 cases of cutaneous leishmaniasis from L. major/ L tropica and twelve cases of visceral infection caused by L. tropica were reported in soldiers from Desert Storm
Endemic Areas for Leishmaniasis BMJ 2003;326:378
Leishmaniasis in the Middle East • 90% of cutaneous leishmaniasis occurs in Afghanistan, Iran, Saudi Arabia, Syria, Brazil and Peru • 8,779 cases were reported in Iraq in 1992 • Sore is commonly called the Baghdad boil • At least 20 cases of cutaneous leishmaniasis were reported in Americans from Desert Storm • 90% of all visceral leishmaniasis occurs in Bangladesh, Brazil, India, and the Sudan • 2893 cases were reported in Iraq in 2001 • 12 visceral leish cases were reported in Americans in Desert Storm • 90% of mucocutaneous leishmaniasis occurs in Bolivia, Brazil and Peru • Rarely associated with L tropica which is found in Middle East
Life Cycle 1- Sandfly bites animal and ingests blood infected with Leishmania 2- Sandfly bites human and injects Leishmania into skin 4- Cycle continues when sandfly bites another human or animal reservoir 3- Another sandfly bites human and ingests blood infected with Leishmania
Cutaneous Leishmaniasis • Most common form • Characterized by one or more sores, papules or nodules on the skin • Sores can change in size and appearance over time • Often described as looking somewhat like a volcano with a raised edge and central crater • Sores are usually painless but can become painful if secondarily infected • Swollen lymph nodes may be present near the sores (under the arm if the sores are on the arm or hand…)
Cutaneous Leishmaniasis • Most sores develop within a few weeks of the sandfly bite, however they can appear up to months later • Skin sores of cutaneous leishmaniasis can heal on their own, but this can take months or even years • Sores can leave significant scars and be disfiguring if they occur on the face • If infection is from L. tropica it can spread to contiguous mucous membranes (upper lip to nose)
Visceral Leishmaniasis • Most severe form of the disease, may be fatal if left untreated • Usually associated with fever, weight loss, and an enlarged spleen and liver • Anemia (low RBC), leukopenia (low WBC), and thrombocytopenia (low platelets) are common • Lymphadenopathy may be present • Visceral disease from the Middle East is usually milder with less specific findings than visceral leishmaniasis from other areas of the world
Visceral Leishmaniasis in Desert Storm The following symptoms were found in eight visceral leishmaniasis patients returning from Desert Storm • Fevers: 6 of 8 • Weight loss: 2 of 8 • Nausea, vomiting, low-grade watery diarrhea: 2 of 8 • Lymphadenopathy: 2 of 8 • Hepatosplenomegly: 2 of 8 • Anemia: 3 of 8 • Leukopenia or thrombocytopenia: 0 of 8 • Elevated liver enzymes: 6 of 8 • No symptoms: 1 of 8 Magill et al, NEJM 1993:328(19)
Visceral Leishmaniasis • Symptoms usually occur months after sandfly bite - Soldiers from Desert Storm presented up to five months after leaving the Persian Gulf • Because symptoms are non-specific and often start after redeployment there is usually a delay in diagnosis • Visceral leishmaniasis should be considered in any chronic FEVER patient returning from an endemic area.
Mucocutaneous Leishmaniasis • Occurs with Leishmania species from Central and South America • Very rarely associated with L. tropica which is found in the Middle East - This type occurs if a cutaneous lesion on the face spreads to involve the nose or mouth - This rare mucosal involvement may occur if a skin lesion near the mouth or nose is not treated • May occur months to years after original skin lesion • Hard to confirm diagnosis as few parasites are in the lesion • Lesions can be very disfiguring
Prevention • Suppress the reservoir: dogs, rats, gerbils, other small mammals and rodents • Suppress the vector: Sandfly • Critical to preventing disease in stationary troop populations • Prevent sandfly bites: Personal Protective Measures • Most important at night • Sleeves down • Insect repellent w/ DEET • Permethrin treated uniforms • Permethrin treated bed nets
Diagnosis • Heightened awareness of individuals, small unit leaders, and medical personnel is critical • Sores that will not heal have to be referred for evaluation – even if not “typical” for leishmaniasis • Individuals with fevers, weight loss, gastrointestinal complaints, anemia, abnormal liver tests should be referred for evaluation • When soldiers present to medical personnel they should volunteer that they were in South West Asia
Diagnosis: Cutaneous Leishmaniasis • Biopsy is required for diagnosis • Biopsy can be done locally if trained medical personnel are available AND Leishmania diagnostic capability present • If trained personnel and diagnostic capability are not available, patient should be referred to Walter Reed Army Medical Center • Biopsy specimens should be sent to Walter Reed (WRAIR) for diagnosis -Leishmania Diagnostics Laboratory - Special laboratories will do microscopy, culture and PCR - Mail out kits/instructions available • Preliminary results should be ready in less than two weeks
Diagnosis:Cutaneous Leishmaniasis Patients with any of the following findings should be referred early to avoid long term complications: • Big lesions (greater than an inch in size) • Many lesions (3 or more) • Sores on the face • Sores on the hands and feet • Sores over joints
Diagnosis:Visceral Leishmaniasis • Must be considered if diagnosis is to be made • Presentation is usually very non-specific and should be considered in febrile patients in / returned from SWA • Antibodies to Leishmania may be present in patient’s serum but this will not confirm or exclude the diagnosis • Diagnosis requires finding Leishmania on biopsy of bone marrow, liver, enlarged lymph node, or spleen • Patients should be referred to a Medical Center, for referral on to Walter Reed Army Medical Center for definitive diagnosis and management if other etiologies excluded
DiagnosisMucocutaneous Leishmaniasis • Early diagnosis and treatment is critical to avoid disfigurement • Patients should be referred to Walter Reed Army Medical Center • Biopsies should be done but require special training to avoid further disfigurement • Biopsies will be evaluated by the same methods and special laboratories as for cutaneous lesion • Because few parasites are present, PCR may be particularly useful
Diagnosis • Mail-out diagnostic kits with instructions are available upon request from the Walter Reed Army Institute of Research • Limited to CONUS facilities and Landstuhl • POC: Dr Coyne/ Dr Weina Phone: 301-319-7155/9956 DSN 285-7155/9956 • Return kit and specimen to: Commander, WRAIR Attn: Leishmania Diagnostics Laboratory Division of Experimental Therapeutics 503 Robert Grant Avenue Silver Spring, MD 20910-7500 • If kit is not available, place biopsy samples in formalin and send for histopathology review. This may be a less sensitive diagnostic method than above.
TreatmentCutaneous and Mucocutaneous • Antimony (Pentostam®, Sodium stibogluconate) is the drug of choice • Given under an experimental protocol at Walter Reed Army Medical Center (WRAMC) • 20 days of intravenous therapy • Available at WRAMC for all branches of the military • Requires patient to come to WRAMC • Fluconazole may decrease healing time in L. major infection • Biopsy and culture to determine species is required • Six weeks of therapy is needed
TreatmentVisceral Leishmaniasis • Liposomal amphotericin-B (AmBisome®) is the drug of choice • 3 mg/kg per day on days 1-5, day 14 and day 21 • Pentostam® is an alternative therapy • 28 days of therapy is required • Although AmBisome® is widely available, the difficulty of accurate diagnosis and the potential severity of visceral infection suggest possible patients be referred to the Leishmania Treatment Center at WRAMC for maximal diagnostic efficiency
Points of Contact • Clinical questions or patient referral LTC Glenn Wortmann, COL Naomi Aronson, COL Charles Oster Leishmania Treatment Center Infectious Disease Service Walter Reed Army Medical Center Comm: 202-782-1663/8695/8691 DSN: 662-1663/8695/8691 • To request Diagnostic Kits CPT Eric Fleming, LTC Peter Weina, CAPT Philip Coyne Walter Reed Army Institute of Research Comm: 301-319-9206/9956/7155 DSN: 285-9206/9956/7155 Email for all is first.lastname@na.amedd.army.mil