Download
1 / 85
850 likes | 1.4k Views
Cutaneous Lymphoid Hyperplasia, Cutaneous T-Cell Lymphoma, Other Malignant Lymphomas, and Allied Diseases. Rick Lin, DO, MPH March 18, 2003. Cutaneous Lymphoid Hyperplasia. Collection of lymphocytes with other inflammatory cells on the skin Maybe monoclonal or mixed with both T or B cells

E N D
Cutaneous Lymphoid Hyperplasia, Cutaneous T-Cell Lymphoma, Other Malignant Lymphomas, and Allied Diseases Rick Lin, DO, MPHMarch 18, 2003
Cutaneous Lymphoid Hyperplasia • Collection of lymphocytes with other inflammatory cells on the skin • Maybe monoclonal or mixed with both T or B cells • Caused by unknown stimuli • Medications, • infections, • insect bites
Cutaneous Lymphoid Hyperplasia • AKA Pseudolymphoma • May progress to lymphoma • Immunosuppression may aggravate the infiltrate and may regress with immunosuppression is removed
Cutaneous B-Cell Lymphoid Hyperplasias • Knowns as Speigler-Fendt sarcoid • Caused by Borrelia, infections, herpes zosters scars, tatoo, drugs • Appears as discrete firm of doughy cutaneous papules or nodules • Most lesions are asymptomatic, treatment not required • If caused by medication, medication should be removed
Cutaneous T-Cell Lymphoid Hyperplasias • Maybe idiopathic • Aka actinic reticuloid and chronic actinic dermatitis • Patient resembles mycosis fungoides • Histologically, dermal infiltrate that is band-like with no grenz zone.
Cutaneous lymphoid hyperplasia • Pseudolymphoma has to be distinguished from cutaneous lymphomas by the combination of clinicopathological correlation, histochemical studies, and, in selected cases, gene rearrangement studies • T cell lymhoma can be usually distinguished from T cell pseudolymphoma by the presence of prominent epidermotropism, large and atypical lymphocytes, and T cell gene rearrangements up to 90%
Cutaneous lymphoid hyperplasia • The lack of acanthosis, "bottom-heavy" infiltrates, light-chain expression of monotypical B-cells, and immunoglobulin gene rearrangements (75%) provide strong evidence for the diagnosis of B-cell lymphoma • A careful monitoring of these patients for the development of lymphoma is necessary
Coalescing erythematous follicular papules and raspberry-like nodules on the right shoulder.
Histological examination of the skin • The microscopic examinations revealed dense and diffuse infiltrates of cytologically benign-appearing lymphocytes and scattered histiocytes in the upper and mid dermis
Immunohistochemical examination of skin. Antibody against CD3+ (T-lymphocytes).
Cutaneous T Cell Lymphomas • Primary Cutaneous T-Cell Lymphomas • Not synonymous with MF • Up to 30% of primary CTCLs are not MF • Primary Cutaneous T-Cell Lymphomas other than Mycosis Fungoides
Primary Cutaneous T-Cell Lymphomas • Primary Cutaneous T-Cell Lymphomas • Mycosis Fungoides • Pagetoid Reticulosis • Sezary Syndrome • Granulomatous Slack Skin • Lymphomatoid papulosis
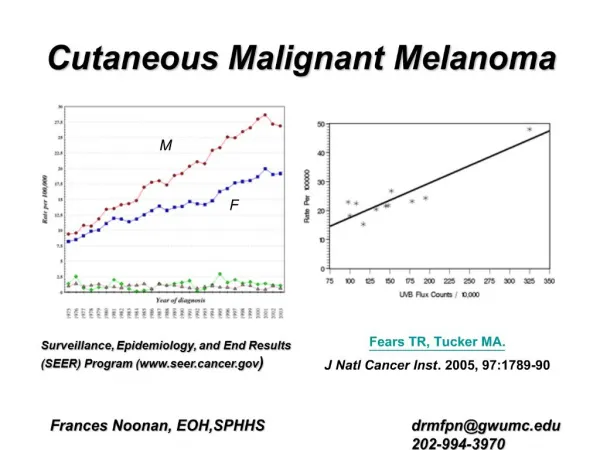
Mycosis Fungoides • Malignancy of T-lymphocytes, almost always MEMORY T-CELL • Black>white • M:F = 2:1 • Race: MF is more common in black than in white patients (incidence ratio 1.6). • Sex: MF occurs more frequently in men than in women (male-to-female ratio of 2:1). • Age: The most common age at presentation is 50 years; however, MF also can be diagnosed in children and adolescents with apparently similar outcomes.
Mycosis Fungoides • Patch Stage – premycotic, severe pruritis. • Plaque Stage – infiltrated plaque • Tumore stage – when de novo, called d’ emblee form • Erythroderma – Rare
MF Staging • TNMB system on skin (T) node (N), viscera (M), and blood (B) • T1 – Skin involvement <10% • T2 – Skin involvement >10% • T3 – Tumor • T4 – Erythroderma
MF Staging • N0 – normal nodes • N1 – palpable but not pathologically MF • N2 – not palpable but pathologically MF • N3 – clinically and pathologically involved • M0 B0 - Viscera and blood not involved • M1 B1 - Viscera and blood involved
MF Staging • Stage IA – T1, N0, M0 – 8-9% progress • Stage IB – T2, N0, M0 – 11-16 years surv • Stage IIA – T1-2, N1, M0 – 7.7 years • Stage IIB – T3, N0-1, M0 – 3-8 years surv • Stage IIIA – T4, N0, M0 – 1.8-3.7 years • Stage IIIB – T4, N1, M0 – 1.8-3.7 years • Stage IVA – T1-4, N2-3, M0 • Stage IVB – T1-4, N0-3, M1
Lymph nodes in MF • Extracutaneous involvement is more clinically evident as the stage and extent of MF increases • Peripheral lymphadenopathy is the most frequent site of extracutaneous involvement in MF • Evaluate palpable lymphadenopathy by obtaining a biopsy because the result influences the patient’s stage, prognosis, and treatment.
MF Workup • CBC – to review the buffy coat smear for Lymph nodes • CMP • Liver Function to include LDH (aggressive) and transaminase (liver involvement) values • CXR • If lymph nodes are palpable • CT to access abdominal and pelvic nodes • Lymph node biopsy
Histologic Findings The criteria for diagnosis include the following: • A bandlike upper dermal infiltrate of lymphocytes and other inflammatory cells, with no grenz zone, is present. • Epidermotropism of mononuclear cells occurs. • When a clear halo surrounds an intraepidermal mononuclear cell singly or in clumps, this is called a Pautrier microabscess. Its presence is suggestive of MF, but it is not necessary for diagnosis. • Little spongiosis of the epidermis is found. • Lymphocytes have nuclei that are hyperchromatic and convoluted or cerebriform.
Pagetoid Reticulosis • Localized epidermotropic reticulosis • Woringer-Kolopp disease • Acral mycoses fungoides • Mycosis fungoides palmaris et plantaris
Pagetoid Reticulosis • 0.6% of all MF cases • Woringer-Kolopp variant: solitary lesion • Ketron-Goodman variant: multiple lesions • Long durantion without progression to frank lymphoma is the clincal hallmark of Woringer-Kolopp • Local excision and radiation therapy maybe curative.
Scan power view. Hyperkeratosis is associated with papillomatosis
Medium power view. Keratinocyte enlargement is seen, and this can occur whenever there is an abnormal cell population in the lower epidermis. Clusters of dark mononuclear cells are in all levels of the epidermis.
High power view. It would be difficult to distinguish between abnormal T cells and small, dark, lymphocytoid melanocytes in this field.
Scattered plaque-like lesions on both lower extremities.Ketron-Goodman disease
Band-like infiltration of lymphoid cells in lower epidermis and upper dermis. Intraepidermal infiltrate were medium- to large-sized atypical cells. Lymphoid cells infiltrating upper dermis revealed no overt atypicality.
Sezary Syndrome • Leukemic phase of mycosis fungoides • Generalized erythroderma, superficial lymphadenopathy, atypical cells in circulating blood • Erythroderma from onset with leonine facies, eyelid edema, ectropion, alopecia, palm and sole hyperkeratosis • Pruritis, burning, chill and profuse sweating
Prognosis • Difficult to treat • Median survival is 3 years • Low dose methotrexate has reasonable response rate of 50% • Photophoresis • Retinoid, interferon alfa, lowdose chlorabucil, prednisone, systemic chemo
Granulomatous Slack Skin • Rare variant of CTCL • Middle-age adult and gradually progress • Erythematous atrophic pendulous redundant plaque • Multinucleated giant cells replaces fat lobules histologically.
Lymphomatoid Papulosis • LyP has a chronic indolent course in most patients; • estimates indicate that as many as 10-20% of LyP patients have a history of associated malignant lymphoma (ALCL, HD, or mycosis fungoides [MF]) prior to, concurrent with, or subsequent to the diagnosis of LyP. • Race: Black persons may be less affected than other racial groups. • Sex: No consistent sex predominance is found in studies. • Age: LyP may develop at any age, usually in the third to fourth decade
Presentation • Primary lesion: Each erythematous papule evolves into a red-brown, often hemorrhagic, papulovesicular or papulopustular lesion over days to weeks. • Some lesions develop a necrotic eschar before healing spontaneously. Occasionally, noduloulcerative lesions may be present • Each papule heals within 2-8 weeks, leaving a hypopigmented or hyperpigmented depressed oval varioliform scar. • Large nodules and plaques may take months to resolve. • Distribution: Characteristically, lesions appear on the trunk and extremities, although the palms and/or soles, face, scalp, and anogenital area also may be involved.
Lymphomatoid Papulosis • Type A: Characterized by large (25-40 mm) CD30+ atypical cells with polymorphic convoluted nuclei and a minimum of 1 prominent nucleolus. These large cells resemble Reed-Sternberg cells when binucleate. Type A LyP is the most common histologic variant. • Type B: Characterized by smaller (8-15 mm) atypical cells with hyperchromatic cerebriform nuclei resembling the atypical lymphocytes in MF. CD30+ large cells are rare, but epidermotropism is more common in this variant.
Lymphomatoid Papulosis • Type C (diffuse large cell type): Characterized by sheets of CD30+ anaplastic large cells
Treatment of LyP • mid-to-high potency topical steroids to hasten resolution. • Low-dose weekly methotrexate is a safe and effective treatment for suppressing LyP; however, the disease recurs within 1-2 weeks after ending medication. • Oral psoralen plus UV-A phototherapy (PUVA) also effectively treats and suppresses the disease. • carmustine, topical nitrogen mustard, intralesional interferon, low-dose cyclophosphamide, chlorambucil, and dapsone help disease suppression.